




5. Vaccination: The Present and Future
The reduction of morbidity and mortality through development of new or improved vaccines continues. In October 1992, vaccination against infection by Haemophilus influenzae type B (Hib), a major cause of meningitis, was included in the childhood immunisation programme in Britain. The effect was immediate, for Hib infections fell by 70% in the period January to March, 1993 (1).
The introduction of the vaccine in Britain was triggered by the outstanding success of the experiment in Finland, where the introduction of the vaccine in 1986 reduced the incidence of Hib menigitis, which had been steadily rising since the 1960s, to zero by 1991 (2) (Fig. 5.1).
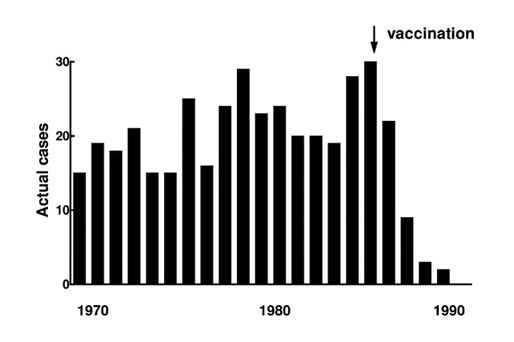
Fig. 5.1 Hib meningitis in Helsinki. Actual cases, 1970-1990.
Similar benefit had been reported in three regional studies of Hib meningitis in the USA, where falls in incidence of between 80-90% occurred over a two year period following vaccination against Hib (3) (Fig. 5.2).
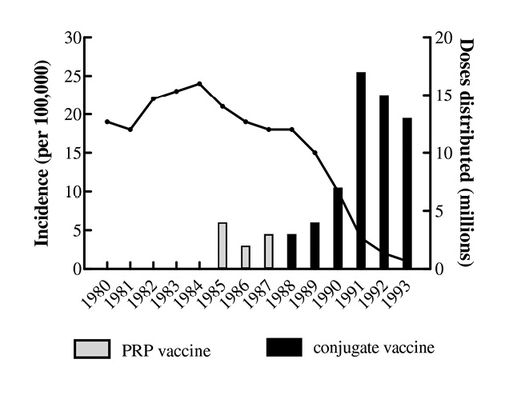
Fig. 5.2 Decline of Hib Meningitis in USA children under 5 years, 1980-1993.
Prior to vaccination, 1500 cases of Hib infection occurred every year in the UK (mostly in children under one year), over half resulting in meningitis. Despite the effectiveness of antibiotics against the bacillus, it killed 65 children and caused permanent brain damage, deafness etc. in a further 150 each year.
The drive to produce a prophylaxis against this potentially devastating disease was considerable, but initial efforts were stymied by the nature of the antigen. This is a polysaccharide present in the capsule of the bacterium, a linear polymer of ribose, ribitol and phosphate (PRP). Antibodies to PRP were effective at passively immunising animals, but PRP vaccines could only produce a poor, short-lived immunity in children under one year, that is those at greatest risk.
After much experimentation the immunogenicity of PRP was increased by coupling it to a protein. This general technique had been suggested by the work of Landsteiner (of blood group fame) and had been shown to be effective in protecting mice against infection with pneumococci (4). Conjugates of PRP with bovine or human albumin, haemocyanin and diphtheria toxoid were shown to be powerfully immunogenic in mice and rabbits (4). From these experimental studies four effective vaccines were developed for human use, based on PRP linked to diphtheria toxoid, tetanus toxoid or a membrane protein from meningococci. Each vaccine was of course subject to the standard animal tests for innocuity.
In terms of extent, malaria is one of the most serious infectious diseases. Actual numbers of those affected are difficult to establish, due to the remoteness of some of the areas where the disease is endemic. A recent estimate suggested that malaria causes 3 million deaths per year in Africa alone, one third of these being children under 5 years of age (5). The parasite is generally developing resistance to antimalarial drugs, as is the anopheles mosquito to insecticides. An effective vaccine has thus long been sought and may now have been found since the prototype vaccine SPf66 has been shown to produce a “strong immune response” in a recent trial in Tanzania (5). SPf66, developed by Patarroyo at the University of Bogota, was perfected by experiments in aotus monkeys (6).
The Future
What next? Will research to produce new vaccines become redundant? Hardly. The spectre of AIDS still looms, other fatal diseases emerge and old diseases re-emerge as problems.
Tuberculosis is on the increase in certain areas and paediatricians are questioning the policy of some health authorities to discontinue routine BCG vaccinations, this despite the advice of the British Thoracic Society to continue to offer BCG to all 10 to 14-year-olds and neonates in areas where the incidence of tuberculosis is high (7).
An emergent problem is posed by hantaviruses. An estimated 200,000 people world-wide become infected with hantaviruses each year, between 4,000 and 20,000 die as a result (8). Hantaviruses, which produce haemorrhagic fever and chronic nephropathy, normally infect rodents, but can easily spread to humans under certain conditions. In October 1993, the US Center for Disease Control and Prevention confirmed that there were 42 cases (with 26 deaths) of a new disease, hantavirus pulmonary syndrome. This had presumably arisen due to the sudden proliferation of the rodent population in SW states caused by unusual social and climatic changes (9). Hantavirus infections are virtually untreatable. The development of a vaccine is the only way to combat the threat of an epidemic.
The denial of the importance of animals in research into the nature and treatment of infective disease, and the insistence of animal rights groups that economic and social change is the sole cause of the decrease in morbidity and death from infection cannot be sustained. The consequent questioning of the effectiveness of vaccination, and the promulgation of unsupportable allegations of the toxicity of vaccines, is at best unjustified and in some instances thoroughly irresponsible (see for example 10).
VACCINES INTRODUCED FOR HUMAN USE.
From Cryz SJ (1991) Vaccines and Immunotherapy. New York: Pergamon.
|
1880 |
|
|
1890 |
|
|
1920 |
|
|
1930 |
|
|
1940 |
|
|
1950 |
|
|
1960 |
|
|
1970 |
|
|
1980 |
An earlier version of this chapter was published as: Vaccination: the present and future. RDS News April 1994 14-15.
References
- Anon (1993) Fall in childhood Hib infection reported. Pharm J 250 633.
- Peltola H, Kilpi T, Anttila M (1992) Rapid disappearance of haemophilus influenzae type B meningitis after routine childhood immunisation with conjugate vaccines. The Lancet 340 592
- Dixon B (1993) Microbe of the month. The Independent, February 8.
- Sood S & Daum R (1991) in Vaccines and Immunotherapy. ed Cryz S. New York: Pergamon.
- The Independent, February 14 1994.
- News and political reviews. Br Med J (1991) 302 432.
- Anon (1993) Fall in childhood Hib infection in USA. Pharm J 251 216.
- Dixon B (1993) Microbe of the month. The Independent, December 13.
- Levins R et al. (1993) Hantavirus disease emerging. The Lancet 342 1292.
- Williams L (1993) A shot in the dark. The Guardian July 20.

