




7. Diphtheria: Understanding, Treatment and Prevention
Diphtheria levies a toll of clinical incidence of 10% of all born with a mortality of 5 to 7 per 1000; immunisation reduces this to an incidence of 1% and zero mortality.
Report of Medical Officers of Health,
Diphtheria Immunisation in Infancy,
The Medical Officer (1932) 48 188.
In the sanitary 1990s it is hard to envisage the experiences of physicians working in the fever hospitals a century ago. Yet this is the only way to appreciate the progress made in the treatment and prevention of infective disease. An inability, or unwillingness, to undertake this exercise largely explains the misrepresentation by some of the value of early treatments of infections. These treatments stemmed from basic research into causative agents and mechanisms of toxicity.
A prime example is diphtheria. The melancholic effect of having to watch a succession of children die either from suffocation or, as the disease progressed, from paralysis and heart failure, was wretched enough. Add to this the demoralisation and sense of impotence caused by the lack of effective treatment, then one can appreciate how dispiriting the practice of medicine could be at that time.
Diphtheria was formally described by Bretonneau in 1826, although epidemics among children of “malignant sore throat destroying life by suffocation and sometimes leaving paralytic sequelae” had been described since earliest times. The epidemics tended to be cyclical “often lasting for many years, and followed by intervals of quiescence” (1).
The primary lesion of the disease occurs in the upper respiratory tract. It is a thick, leathery, bluish-white pseudomembrane composed of bacteria, dead cells and fibrin. Should the lesion occur in the laryngeal region, the airway may become occluded and intubation would therefore be necessary.
The emergence of the germ theory triggered the start of the scientific investigation of the aetiology of diphtheria. Klebs in 1883 described a bacillus obtained from the pseudomembranes of diphtheria patients. The straight or slightly curved rods described by Klebs we know today were indeed Corynebacterium diphtheriae, although Klebs’ study was purely morphological. A year later Loeffler isolated and cultured the bacillus from 13 undisputed cases of diphtheria. When the cultures were inoculated onto injured mucous membranes of various animals, pseudomembranes developed, resembling those in patients. Nevertheless, Loeffler’s report was somewhat reserved, since he was unable to explain the systemic symptoms of diphtheria.
In both animals and man infected with the supposed causative organism there are severe systemic disturbances and even organ degeneration, but the bacillus could be found only in the local lesion.
The anomaly was resolved in 1888 by the observation by two of Pasteur’s colleagues, Roux and Yersin, that the broth used to grow the cultures of bacillus diphtheriae remained toxic for guinea pigs after the bacteria had been removed by filtration. The filtered broth was also shown to be toxic for rabbits, dogs, cats and horses (2). Thus the systemic symptoms of the disease were due to the absorption of a toxin exuded during the growth of the bacilli on the mucous membrane. This observation was very important, since studies on hog cholera in 1885 had demonstrated that administration to an animal of very small concentrations of a bacterial product could eventually produce immunity to that infection. Consequently in 1890, von Behring and Kitasato were able to show that administration of very small amounts of diphtheria toxin to animals resulted in the presence in their plasma of a factor which, when mixed with the toxin, rendered it innocuous to animals (3).
The subsequent observation that this plasma, when actually administered to animals, could protect them from fatal doses of diphtheria toxin paved the way for the use of “diphtheria antitoxin” to treat diphtheric patients. According to most accounts the first clinical use of the antitoxin was in Berlin on Christmas Eve 1891, when von Behring administered it to a seriously ill girl who subsequently recovered (Fig. 7.1).

Fig. 7.1 1909 photo of Emil von Behring (1854-1917). Wellcome Library, London, CC BY.
To produce an effective antitoxin, a potent toxin was required. Typically, a virulent strain of bacillus was grown on a shallow layer of medium and, after 6-8 days, the formed toxin was obtained by filtration. The toxin could only be standardised by a biological assay. This was the measurement of the volume of filtrate that would kill a guinea pig of 250g body weight within 5 days. The lethal volume was required to be below 0.1cc for the toxin to be of adequate strength (4).
The antiserum was usually produced in horses. Gradually increasing subcutaneous doses of toxin were administered over a period of 2-3 months. At the end of this time the horse plasma contained possibly 1,000 antitoxin units per cc and the animal could continue to provide antitoxin for 2-4 years.
The antitoxin in turn required standardisation. This was achieved by comparing its ability to render a sample of toxin innocuous to guinea pigs, with that of a stable, standard sample of antitoxin provided by a central source (4).
Serotherapy in Diphtheria
After the first successful treatment of diphtheria with the antitoxin by von Behring, the use of equine diphtheria antitoxin spread rapidly. Even today serotherapy is the only way to avoid the severe effects of systemic intoxication.
Early on it was realised that to be effective the antitoxin had to be administered early, since the toxin could only be neutralised before it became bound to the tissue elements where it caused toxicity. Rabbits given a tenfold lethal dose of diphtheria toxin could be saved by a relatively small dose of antitoxin if it was administered shortly after the poison. If the injection of the antitoxin was delayed, then increasing doses were required to prevent death. If the administration of the antitoxin occurred after one hour, then no dose would save the animal (4).
Clinical Effects of the Antitoxin
In 1894, Roux and co-workers published their report of the striking benefit produced by antitoxin treatment of diphtheric cases admitted to the Hospital for Sick Children in Paris (5) (Fig. 7.2).
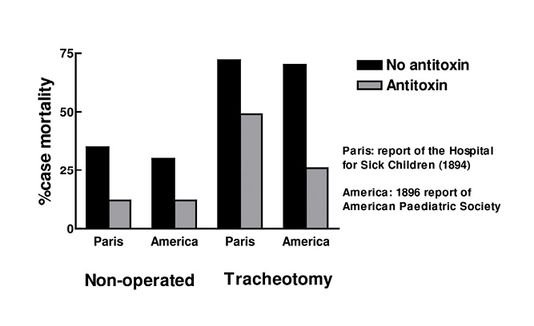
Fig. 7.2 Effect of antitoxin on case mortality.
The serum was administered to every case proved by bacteriological examination to be diphtheric, during February to July 1894. Between 1890-1893, before treatment, 3,971 children were admitted, 2,029 of whom died, a case mortality of 51%. During the first 6 months of serum treatment 448 children were admitted of whom 109 died, a case mortality of 24.3%. During the same period, Trousseau Hospital in Paris was not using the antitoxin, 520 cases were admitted there, 316 died, a case mortality of 60%.
In some cases, where the lesion extended to the laryngeal region, tracheotomy was required. Case mortality in these instances was 73% in the Hospital for Sick Children prior to the use of antiserum. During the trial period this was reduced to 49%, whereas at the Trousseau Hospital the contemporary mortality in such cases was 86%.
After Roux’s signal paper, the use of diphtheria antitoxin spread throughout the developed world. Wherever it was used there occurred a reduction in case mortality. Although there was nothing akin to a double-blind clinical trial (case mortalities were compared to those prior to the adoption of the antitoxin) the circumstantial evidence was compelling. Amongst many anecdotes is the oft quoted report of the problem at Baginsky’s clinic in Berlin, where they were unfortunate to run out of the antitoxin and the case mortality immediately rose from 15.6% to 48.4% (6).
Based as it was firmly upon experiments in animals, predictably the use of the antiserum came under attack from the antivivisection community. Even as recently as 1934, Beddow Bayly alleged that the antitoxin could not work, since the disease was not caused by the Klebs-Loeffler bacillus but by “drain poison” (7). Strangely, in the same publication he asserts, through selective quotation, that the apparent drop in mortality following the use of antiserum occurred because of diphtheria diagnosis by bacteriological means, i.e. by demonstration of the presence of the bacillus in throat swabs. The result of this was that very mild cases, which previously would have been recorded as minor sore throat, were diagnosed as diphtheria. Beddow Bayly asserted that the inclusion of these mild, self-limiting cases falsely reduced the case mortality. Firstly, this ignores the fact that the reduction in mortality immediately followed the introduction of the antitoxin treatment, whereas the bacillus had been described 10 years previously. Secondly, it takes no heed of the striking reduction in mortality of cases which required tracheotomy, and thus were of undoubted severity. Finally, there were many studies that demonstrated the necessity to administer the antiserum as early as possible, mortality increasing as the treatment was delayed from the first to the fifth day of the disease. As Sir Charles Martin, an authority on the treatment of diphtheria, emphasised: “If the antitoxin were a remedy of no value, whether it were administered on the first or the fifth day of the disease would be immaterial” (8).
Acceptance of the antitoxin was lukewarm in Great Britain. It was not widely used until the publication in 1898 of the report by the Special Committee, set up by the Clinical Society, to investigate the efficacy of antitoxin treatment of diphtheria (9). The report compared 633 treated cases with 3,042 cases that did not receive antitoxin. The 50-page report concluded:
- General mortality is reduced by one-third
- Mortality in tracheotomy falls by one-half
- Extension of the membrane to the larynx very rarely occurs after administration of the antitoxin
- Duration of life in the fatal cases is prolonged
- The number of fatal cases is less when antitoxin is used early in the illness than in those that do not receive it until a later period.
Even after large doses there were no serious ill effects. Rashes occurred in one third of cases. Pain and swelling of the joints were produced in a number of cases.
Immunisation against Diphtheria
As emphasised by Cobbett in 1933 (10), the benefit produced by the antitoxin was “by no means to be despised,” but it was only able to reduce the overall case mortality to a certain percentage. This was partly due to the practice of relying on bacteriological diagnosis before administration of the antitoxin, thus delaying the early use of the remedy, when it is most efficacious.
In 1890, von Behring and Kitasato had mooted the possibility of generating active immunity against diphtheria, and had actually produced immunity in guinea pigs by the use of a “detoxified” diphtheria toxin. Some years later, von Behring (11) produced a long-lasting immunity in guinea pigs, monkeys and asses by using a carefully balanced mixture of toxin and antitoxin (a technique which had been used with success in New York for the generation of antitoxin in horses). The toxin/antitoxin mixtures were used in limited studies by von Behring to protect humans against diphtheria, but widespread immunisation only began with the development of formalin-inactivated toxin, introduced independently by Glenny and Hopkins (12) and Ramon (13).
The formalin-inactivated toxoid (and the later alum precipitated and adsorbed diphtheria toxoids) were required to be standardised for antigenic potency by measuring their ability, 28-30 days after inoculation, to protect guinea pigs against a challenge with a 20-fold LD50 of a suitable diphtheria toxin. Innocuity tests also had to be performed to exclude dermal toxicity (intracutaneous injection to rabbits or guinea pigs – observed for 48 hours) and delayed, systemic toxicity (parenteral administration to guinea pigs – observed for 6 weeks) (14).
The adoption of immunisation against diphtheria occurred in piecemeal fashion, its initiation depending on the awareness and energy of individual Medical Officers of Health. There was also a vociferous opposition both from the antivivisection movement and the National Anti-Vaccination League.
From early studies in restricted populations it emerged that sanitary measures of isolation would be of limited value in the containment of diphtheria, since the Health Committee of the League of Nations demonstrated that 97% of infections were not contracted from clinically evident cases of the disease, but from the more numerous healthy carriers of virulent bacilli (8).
The dramatic impact of immunisation was cogently illustrated by the well- controlled investigation of the incidence of cases of diphtheria at Greenwich Hospital School, where immunisation abolished the disease despite the fact that infective but healthy carriers were present in constant numbers both before and after the inoculation programme.
Similarly, striking evidence for the benefits of immunisation against diphtheria comes from the clear protection of nursing and auxiliary staff afforded by inoculation of those deemed to be at risk (i.e. those with a positive Schick test) in diphtheria hospitals (15). Non-immunised staff were 14 times more likely to contract the disease as the inoculated.
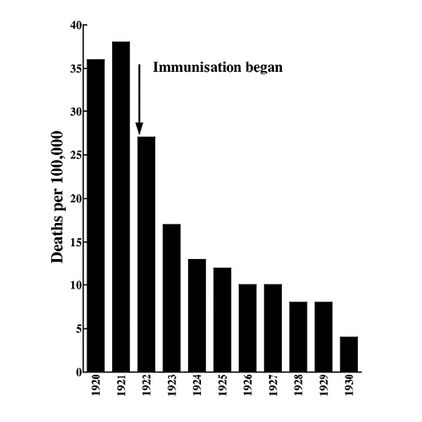
Fig. 7.3 Diphtheria death rate in New York, 1920-1930.
Even in field trials, the benefits of inoculation were clear, for example in New York (described in 1932 as the “best immunised city in the world” (16; Fig. 7.3)) and in Birmingham, which was one of the earliest English cities to institute diphtheria immunisation in 1926. Here a marked decline in incidence of diphtheria was seen by 1931, when almost 10% of children had been vaccinated (17) (Fig. 7.4).
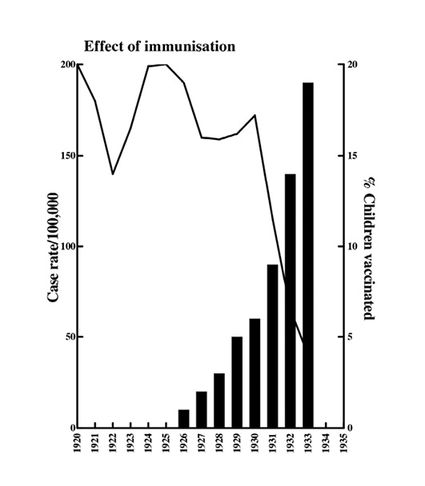
Fig. 7.4 Incidence of diphtheria in Birmingham (children 5-14 years), 1920-1935.
Despite the clear medical evidence of the protection offered by inoculation, the Anti-Vaccination League fought a vigorous rearguard action, disagreeing with immunisation “by filthy concoctions produced from the artificially diseased blood of the lower animals being injected into the clean blood stream of human beings” (18). (The vaccine of course was simply the formalin-treated toxin, it was not obtained from an animal). Much was made of the supposed toxicity of the vaccine (19), although at the time this battle was at its height (1932), 150,000 persons in Great Britain and Ireland had been immunised against diphtheria without any ill-effect, let alone fatality (20).
The success in local health districts of inoculation against diphtheria resulted in the acceptance across Britain of the immunisation of pre-school children in 1940. The drop in incidence of the disease after this is an impressive illustration of its efficacy (Fig. 7.5).
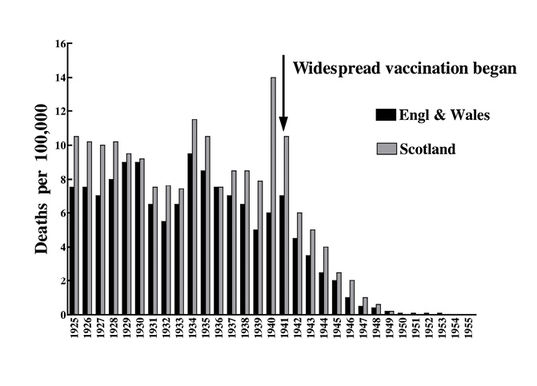
Fig. 7.5 Diphtheria death rate in Great Britain, 1925-1955.
The success of the many local experiments into the protection offered by diphtheria immunisation means there can be no doubt that this technique is effective in reducing the incidence and mortality of the disease. However, as the WHO statistics show (21), in several European countries significant declines in death rates have been registered, despite the fact that in these countries only a few vaccination programmes were carried out in limited areas. It is thus possible that a concurrent change may have taken place in the pathogenicity of Corynebacterium diphtheriae, or human resistance may have increased.
It is known that with the increase in the number of resistant individuals as a result of immunisation, the toxinogenic C diphtheriae becomes replaced by nontoxinogenic strains in carriers. It is possible this could account for the general decline in diphtheria morbidity.
Could Diptheria Return?
The report of a serious case of diphtheria in a Finnish man, contracted during a trip to Russia, has resuscitated interest in the need for booster vaccinations (22). This particular patient entered hospital during Easter 1993, developed neurological symptoms (paraesthesia of right mandibular area and loss of power in all four extremities) and signs of myocardial toxicity. He was still in hospital at the time of the publication of the case (July 1993). The absence of the toxinogenic strains in countries where inoculation was widespread means that one does not acquire booster protection by natural infection. It may thus be necessary to reinforce protection, particularly for those travelling to countries endemic for diphtheria. The non-toxic, antigenic cross reacting materials (CRM), obtained after random mutagenesis of the TOX gene, may be developed as suitable alternatives to the toxoid vaccines (23), which may cause untoward reactions in adults.
The occasional case of diphtheria that occurs intermittently in Europe, serious as each is, serves as a reminder of how far we have progressed from the dire situation in the diphtheria wards one hundred years ago.
An earlier version of this chapter was published as: Diphtheria – understanding, treatment and prevention. RDS News January 1994 8-12.
References
- Whitelegge BA, Newman G (1893) Hygiene and Public Health. 2nd ed, London: Cassell.
- Roux E, Yersin A (1888) Contribution à l’étude de la diphthérie. Ann l’Inst Pasteur 2 629-61.
- Behring von E, Kitasato S (1890) Ueber das Zustandekommen der Diphtherie-Immunität und der Tetanus-Immunität bei Thieren. Deutsch Med Wochensch 16 1113-14.
- Zinsser H (1931) Textbook of Bacteriology. 6th ed, New York: Appleton.
- Roux ME, Martin ML & Chaillou MA (1894) Trois cents cas de diphtérie traités par le sérum antidiphtérique. Ann l’Inst Pasteur 8 640-61.
- Paget S (1906) Experiments on Animals, 2nd ed, London: Nisbet.
- Beddow Bayly M (1934) The Schick Inoculation for Immunisation against Diphtheria. BUAV and the National Anti-Vaccination League.
- Rogers L (1937) The Truth About Vivisection. London: Churchill.
- (1899) Report of the Special Committee on Diphtheria Antitoxin. Trans Clin Soc 31 1-50.
- Cobbett L (1933) The decline in the death rate of diphtheria compared with that of scarlet fever. BMJ ii 139-40.
- Behring von E (1913) Ueber ein neues Diphtherieschutzmittel. Deutsch Med Wochenschr 39 873-76.
- Glenny AT & Hopkins BE (1923) Diphtheria toxoid as an immunising agent. Br J Exp Pathol 4 283-288. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2047731/
- Ramon G (1924) Sur la toxine et sur l’anatoxine diphthiriques. Ann l’Inst Pasteur 38 1-10.
- (1953) Diphtheria and Pertussis Vaccination WHO Technical Report Series No 61. http://whqlibdoc.who.int/trs/WHO_TRS_61.pdf
- Harries EH (1939) Control of the common fevers: diphtheria. The Lancet i 45-48.
- (1932) Report of Society of Medical Officers of Health. The Medical Officer 48 188.
- Burn M & Fellowes V (1934) Diphtheria immunisation: a review of eight years work in Birmingham. The Lancet ii 1181-85.
- Clayton Smith A (1932) Letter to Yorkshire Observer, May 17.
- Clayton Smith A (1932) Letter to Yorkshire Observer, May 24.
- Greenwood Wilson J (MOH, Dewsbury) (1932) Letter to Yorkshire Observer, May 21.
- WHO (1951) Epidemiology and Vital Statistics Report. 4 92-111.
- Lumio J, Jahkola M, Vuento R, Haikala O & Eskola J (1993) Diphtheria after visit to Russia. The Lancet 342 53-54.
- Cryz SJ (1991) Vaccines and Immunotherapy. New York: Pergamon.

