8. Investing in Health
© Pierre-Yves Geoffard, CC BY 4.0 https://doi.org/10.11647/OBP.0280.08
Introduction
Broadly speaking, any healthcare intervention that improves patients’ health may be qualified as an investment. Good health, a major component of individual welfare, may also increase labour supply, especially during older age, as well as increasing labour productivity. In that sense, health is a key component of human capital. In the words of the European Commission (2014), “the Commission adopted the SWD “Investing in health” (as part of the Social Investment Package, SIP) which presents health as a value in itself and as a “growth-friendly” investment.” In line with this definition, the Commission recommended in 2014 “investing in three key areas: health systems sustainability, people’s health as a human capital, and reducing health inequalities.”
However, such an approach raises many issues. Not every good or service that improves welfare may be qualified as an investment. Many healthcare treatments may alleviate pain, and improve or restore the autonomy of the patient treated, without increasing their future productivity. The value of healthcare cannot be reduced to the effect it may have on future production, and benefit/cost analysis now defines the benefit of healthcare as the gain it provides in terms of quality of life or longevity. We choose, in this chapter, to focus on a narrower definition of health investment: current expenditures that may improve the future production of health. Such a definition encompasses the prevention of diseases, human capital investment in healthcare and the long-term care labour force, and capital expenditure in healthcare. Put differently: “How much a country invests in new health facilities, the latest diagnostic and therapeutic equipment and information and communications technology (ICT) can have an important impact on the capacity of a health system to meet the health needs of the population and thus contribute to better outcomes” (OECD 2019).
When we talk about health and healthcare, some contextual elements are important to keep in mind.
8.1 Health
After decades of constant improvement, the decrease of mortality in most European countries, especially the richest ones, has been slowing down in the recent period. Indeed, in 2015, overall mortality even increased across Europe, due to a severe influenza outbreak which killed many elderly individuals. Overall, population ageing and increases in obesity and diabetes slow down the decreasing trend of mortality by stroke or heart disease. Chronic diseases not only increase mortality, but they also reduce quality of life, especially at older ages. Population ageing also raises important issues in terms of health and long-term care, as in many countries, gains in life expectancy are no longer associated with gains in life expectancy with good health. Moreover, in all countries, individual health is strongly associated with socioeconomic status: the richer and the better educated live longer, and in better health, than the poorest and the least educated. Last but not least, the COVID-19 pandemic has induced, between March 2020 and June 2021, more than 735,000 deaths in the European Union alone.
In short, there have been as many important progresses as there are challenges ahead. Medical innovation has been incredibly successful in discovering several vaccines against COVID-19 in a few months, but better treatments for acute cases are still needed. More generally, as chronic diseases are becoming more and more prevalent, and as more and more hospital treatments can now be administered in ambulatory care units, healthcare systems need to evolve from hospital-centered organisations to more decentralised ones, which raises important issues in terms of coordination of care. The increase in “behaviour-related” diseases―such as those induced by lack of physical activity, alcohol or other drug consumption, and unhealthy diets―require public health interventions, all the more so as these diseases and these behaviors reveal strong social inequalities. Other evolutions of healthcare also impact investment, both actual and needed. New medical treatments, especially gene therapies and recent advances in oncology, often come at a very high unit cost. Finally, the digitalisation of health and healthcare information creates new possibilities for improving patients’ follow-ups and healthcare coordination.
8.1.1 Healthcare and Investment in Healthcare
Overall, in 2018 European Union countries spent 10% of their GDP on healthcare,1 and this figure varies from 5.7% in Luxemburg to 11% in Germany, France, or Sweden. Hospital care accounted for 36% of healthcare expenditures, ambulatory care for 25.5%, and drugs and medical devices represented 17.6%. Labour costs represent about three quarters of hospital and ambulatory care costs, and an even larger share of long-term care costs.
Investment in healthcare capital typically represents a small share of healthcare expenditures, highly variable across countries and time (Figure 1).
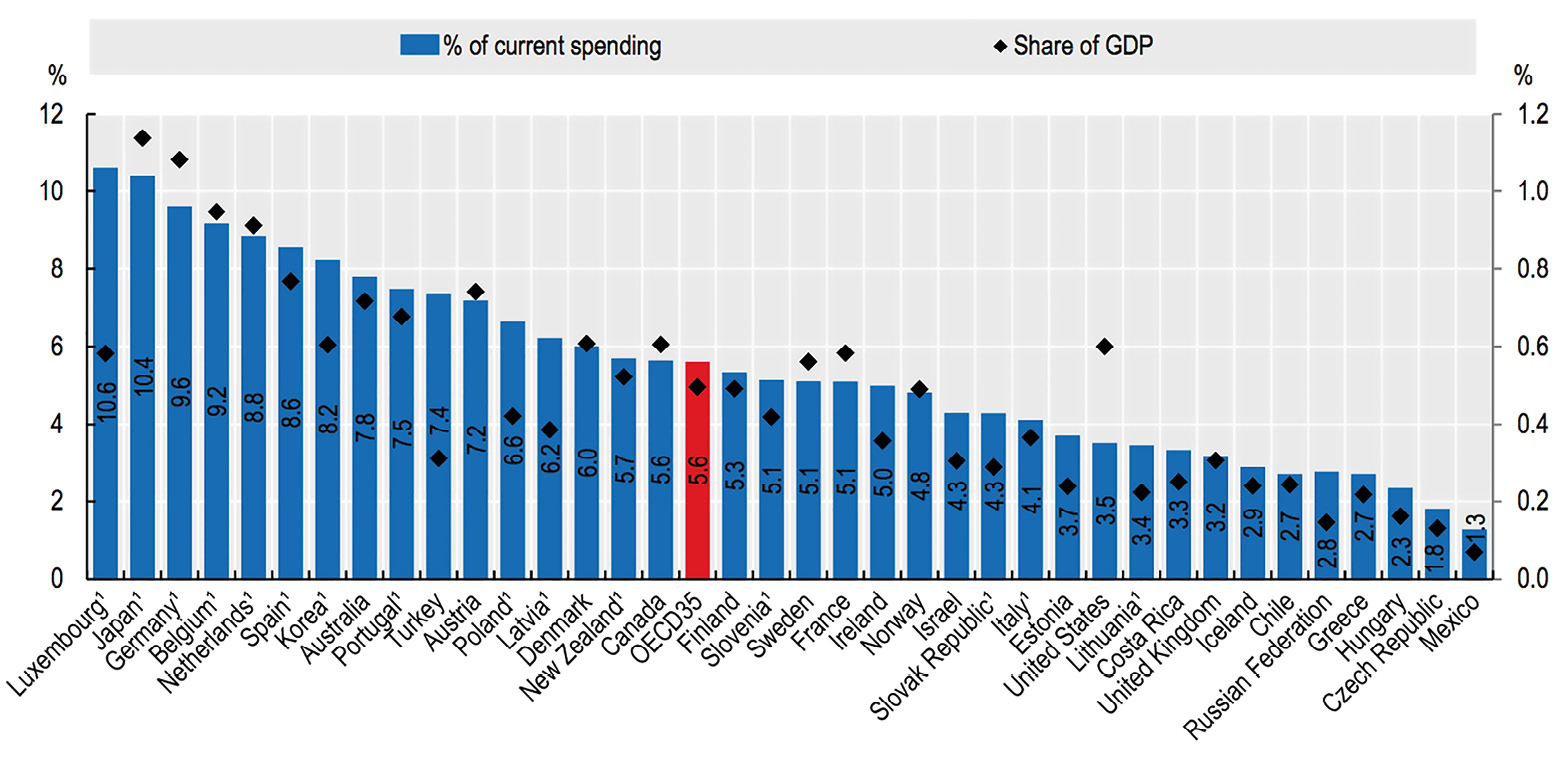
Fig. 1 Investment in Healthcare Capital as a Share of Current Health Expenditure, 2017 (or Nearest Year).
Source of data: OECD 2021, Health at a Glance.
8.1.2 Recent Crises
The Global Financial Crisis of 2008 induced tension on public budgets, including healthcare financing, due to a decrease in revenues following a decrease in economic activity. Given the high share of labour costs in healthcare, and given that these costs are mostly fixed in the short run, the pressure on healthcare budgets led to a substantial drop in investment in some countries, especially Greece and the UK.
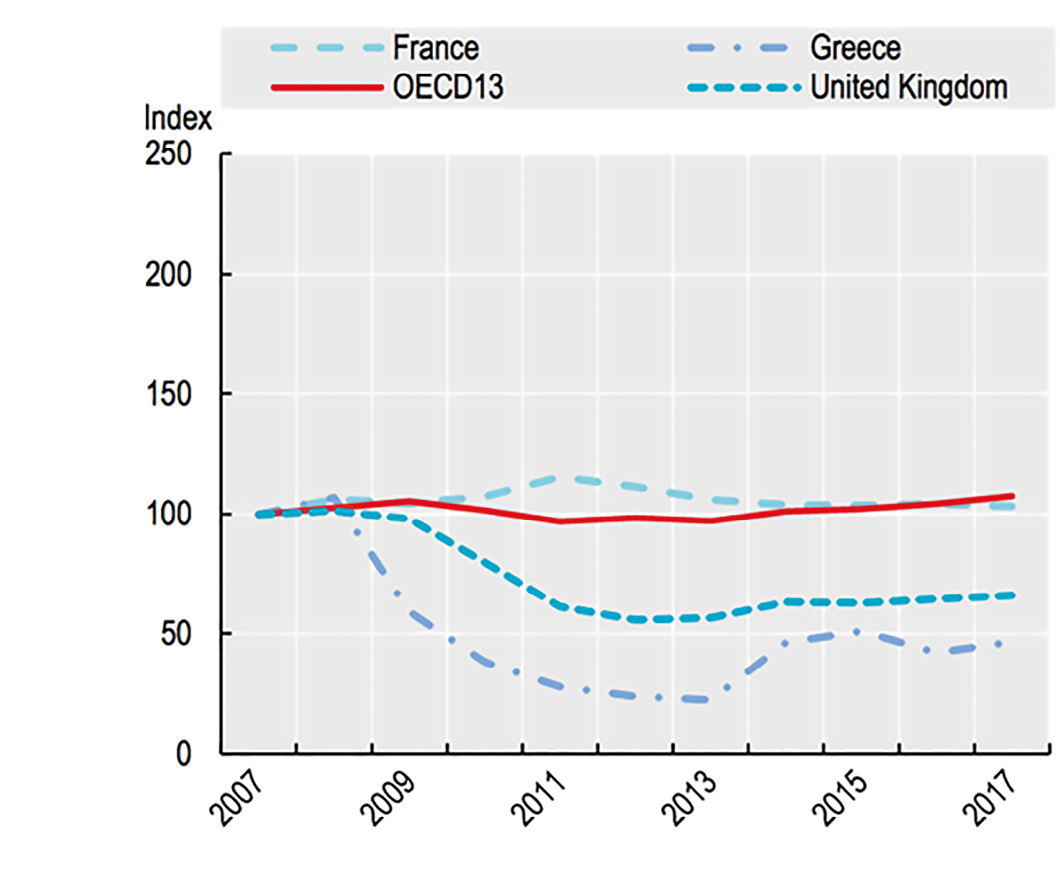
Fig. 2 Trends in Healthcare Capital Expenditure.
Source of data: OECD Health Statistics 2019, OECD National Accounts.
The COVID-19 pandemic induced high-excess mortality among the elderly. The large number of patients requiring intensive care for unusually long hospital stays put tremendous pressure on hospitals. In order to cope with an exceptionally large number of COVID patients, most hospitals postponed non-urgent care for other diseases, which increased treatment delays. The structure of healthcare expenditures changed, with a sharp decrease in ambulatory care, important changes in medical drug consumption, and (of course) increases in hospital care costs; given these rapid and contrasted evolutions, it is still too early to say how much total healthcare expenditure has increased by. However, the sharp drop in GDP, induced both by individual responses to the risk of infection and by policy interventions such as lockdowns and other restrictions on social and economic activity, led to a sharp decrease in healthcare financing revenues, which are highly sensitive to GDP. As for public budgets, healthcare financing experienced in 2020 a historical deficit, contributing to a strong increase in the “social debt”.
8.2 Relevant Investment in Health and Healthcare
However, it may be worth reminding that investment decisions should be based on the balance between current costs and the prospect of future benefits, and not on currently available budgets. This section suggests some areas in which investing resources may improve healthcare systems in the future, including investment in preventing future diseases. These suggestions are highly subjective, and each of them would require a thorough benefit/cost analysis which would go way beyond the scope of this brief.
8.2.1 Human Capital
As stated above, healthcare principally involves labour. Training medical staff usually takes up to ten years or more, taking into account medical school, internships, residencies, and specialisation. In a context in which healthcare organisations, due to digitalisation, switch from hospital to ambulatory care, and in which there is growing importance of chronic and older-age diseases, investment has to be made now to train the physicians that we will need in ten years. In addition, medical doctors are not the only workers in the health sector. Population ageing, given the uncertainty about the health condition in which individuals will spend the last years of their life, will induce a strong increase in long-term care needs. Many countries, not only in Europe, already face difficulties in hiring well-trained professionals. As suggested by some2, this challenge may be solved by selective immigration. However, high unemployment rates, especially among women, may also suggest that an increase in training capacities may contribute to solving this challenge. Indeed, if we fail to increase labour in long-term care facilities, the elderly who suffer some loss of autonomy will be taken care of by their relatives—in practice, most of the time by their daughters or daughters in law, some of whom may have to reduce labour force participation in order to be able to devote sufficient time to their parents. Investing in training for long-term care jobs may therefore not only impact long-term care itself, but also female employment in many sectors.
8.2.2 Digital Transformations
Information is central to healthcare production. An episode of care starts with a medical visit in which a physician has to transform some information (symptoms, biological tests, past medical history, etc.) into another form of information (diagnosis). Given the rapid expansion of medical knowledge, every physician has to spend a substantial and growing share of their time learning about new therapeutic opportunities. Information technologies can be of great help, by offering computer assistance to medical decision-making. In some areas (e.g., radiology), systems based on artificial intelligence, relying on the standardised analysis of thousands or more past cases, can produce a highly reliable diagnosis. It is hard to believe that such technologies will not provoke dramatic changes in medical care, and increase healthcare productivity. Such systems are still in their infancy, and will need important investment to generate their full potential.
What is true for medical decision-making is also true for surgery. Surgeons increasingly rely on robots, not as substitutes of their own practice, but as a complement to it. For instance, a high-speed connection may allow a surgeon to command a surgical robot at long distance. Additionally, a robot commanded by a surgeon can be more precise than the same surgeon’s hand in executing very precise surgical gestures. Again, such technologies will experience major improvements in the years to come, if they benefit now from relevant investment.
Electronic health records constitute another opportunity for improving healthcare. A typical healthcare episode, especially when it includes some hospital care, involves several physicians, and even more other healthcare professionals. Electronic health records may contribute to a better coordination of all. This is easier to say than to do, however, as many attempts to set up such systems on a large scale have failed in the past. Nevertheless, it is reasonable to believe that they will play an important role in improving healthcare, provided that relevant investment is undertaken.
Information and communication technologies also create the possibilities of improving surveillance and follow-up of chronic patients. For instance, a house may be equipped with sensors that detect the fall of a fragile patient and send an alarm, or measure blood pressure or other elements, the evolution of which may indicate that some action is needed. Again, such technologies are in their infancy, but their potential is huge.
Yet another area in which the digitalisation of health and healthcare creates new opportunities is the value assessment of drugs and medical devices. The producer of a new drug has to prove, in order to bring the drug to the market, that it is safe, and that it improves patients’ health. This proof is usually produced in randomised clinical trials, which impose increasing development costs and delays. Whereas such procedures do increase safety and confidence in efficacy, these delays may be detrimental to patients who have to wait before being allowed to receive the treatment. Once the drug can be prescribed, it remains under strict surveillance, and eventual side effects, too rare to be observed in a clinical trial involving a few hundred or thousand carefully selected patients, can arise when the drug is prescribed in real life to much larger, and more heterogenous, groups of patients. Investing in health data systems that routinely collect information relevant to the evaluation of safety and efficacy of a drug may actually decrease substantially the relative costs of such “real life” experience vs ex ante (in an RCT) production of information.
This issue is particularly relevant for treatments of rare diseases. A disease is qualified as “rare” when it concerns a small number of patients, i.e., when its prevalence is very low, lower than one case per 2000 individuals (actual thresholds vary, but this value is commonly used in Europe). There are many rare diseases, 70 to 80% being genetic diseases, so that the total number of patients suffering from a rare disease is estimated to be around 250,000 in Europe.3
Rare diseases raise important issues in terms of innovation (see Section 8.3. below), and also in terms of health technology evaluation. First, the small number of patients in a given country makes it almost impossible to set up a standard randomised clinical trial with sufficient statistical power. Second, especially for gene therapies, the potential benefit to patients may last for many years, ideally for life, but at the time the therapy is discovered there is a high uncertainty about its duration, and therefore its expected overall value. Third, the unit production cost of such therapies is very high, usually larger than €1 m for the first cases, and given the small prevalence, the possibility to amortise research costs is limited. These elements raise specific issues in terms of pricing, financial risk-sharing between healthcare financing institutions and producers, and patients having access to promising treatments, as there is usually no therapeutic alternative.
A European perspective could bring important benefits: registers of all European patients could be created and maintained, gathering clinical and patient satisfaction data in a standardised way, matched with existing healthcare data such as reimbursement or cost data routinely collected by health insurance organisations. Given that such processes are currently defined and operated at each country’s level, building a European platform will raise important technical, and political, issues.
8.3 Hospital and Long-Term Care
Hospital care is a highly innovative industry. Surgeons can be assisted by surgical robots for many interventions, and sometimes such robots can be operated at long distance. Less invasive surgical procedures can treat patients who now need to stay hospitalised for a shorter period. Some surgical interventions can even be done in the outpatient section of the hospital patients can also be treated at home for illnesses that required full hospitalisation not long ago. Digitalisation offers opportunities to improve coordination of care by providing us with better circulation of information. A reasonable prediction is that fewer hospital beds will be needed in the future, but these beds may be occupied by patients receiving more intensive care.
Needless to say, all such innovations may lead to important changes in the role of hospitals within the healthcare system. Such transformations may require important investment. Identifying the relevant investments which are needed in Europe would go far beyond the scope of this brief, in part because the current state of hospitals varies a lot across, and within, European countries. Relevant innovations may be quite different across, say, northern Italy, Switzerland, and Scandinavian countries, or across southern Italy, Greece, or the United Kingdom. But what is quite clear is that no country will be prepared to face the challenges raised by the transformation of hospital care without important investment.
Population ageing has been associated with some medical progress, but the reduction in mortality at older ages is not necessarily associated with a gain in quality of life in the last years of life, especially for women. Given the sharp increase in the number of elderly people, especially in countries with a low fertility rate and very limited immigration flows, more long-term care homes will need to be built, equipped with medical facilities, and staffed with medical and paramedical personnel. This can be a highly profitable investment, since as stated above, the alternative is to rely on family or informal care to provide long-term care, which in most cases leads to relying on women, some of whom may have to withdraw, temporarily or permanently, from the labour force.
8.4 Industry: Pharmaceuticals
Along with the information technology industry, the pharmaceutical industry is the most intensive in research and development, and about 10% of firms’ revenue is devoted to it on average. It is a key player in a system which articulates fundamental research, usually undertaken in publicly-funded universities; start-ups which often originate from such universities; patent law which grants temporary monopolies to inventors; big pharmaceutical firms which may conduct their own R&D, invest in start-ups, and buy (and sell) patents; health authorities which assess the safety and efficacy of new treatments; healthcare financing institutions which reimburse treatments; and patients who may benefit from new treatments. Research and development by private firms is often subsidised by governments, and innovative financing mechanisms, such as advanced market commitments (Kremer et al. 2020), also contribute to the evolution of cost- and risk-sharing between different bodies.
Public funding of R&D in health technologies varies substantially across countries in Europe, and shows divergence between countries (Figure 3). Public investment in universities, by financing fundamental research in life sciences, also varies substantially. There is high potential in investing more in R&D, both at the fundamental stage of research and in supporting and incentivising private firms.
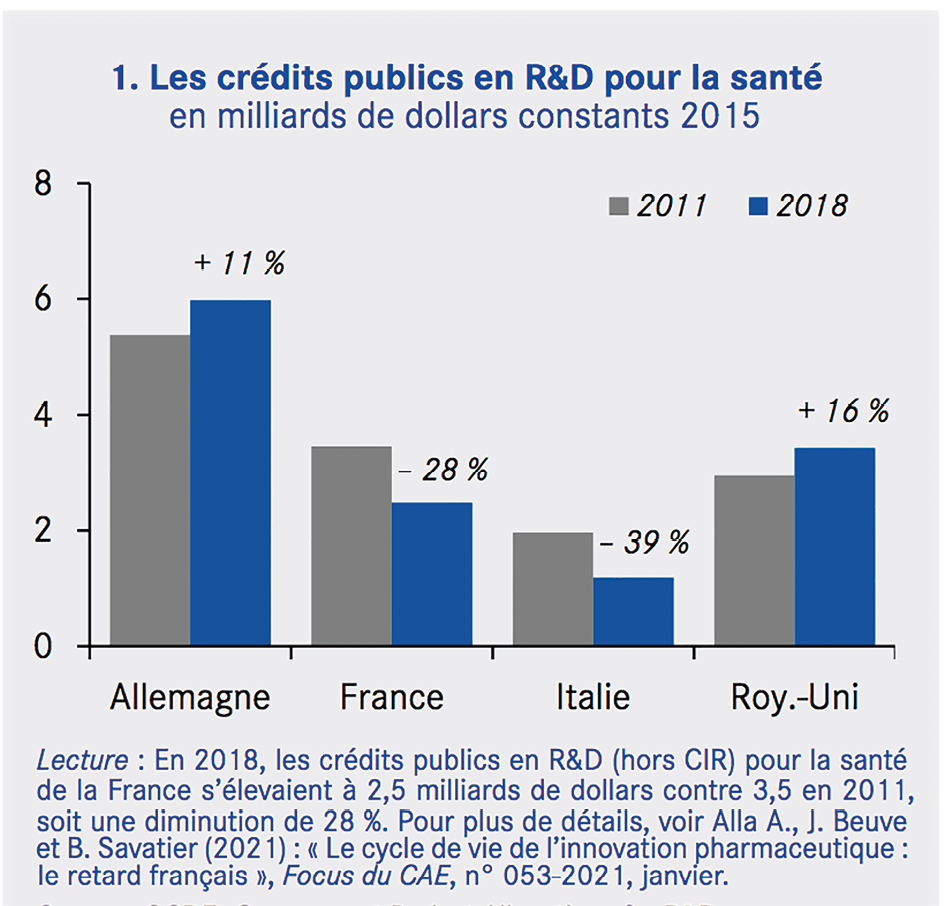
Fig. 3 Public Investment in Healthcare R&D.
Source of data: OECD, Government Budget Allocations for R&D, https://stats.oecd.org/Index.aspx?DataSetCode=GBARD_NABS2007.
Patent protection and drug pricing are also important drivers of innovation. The question seems, at first, not to be related to investment, but it is in fact closely linked. Patent protection and adequate pricing guarantee profits over ten or more years, and this perspective of profits stands as a strong incentive to innovate―and to put more effort into―therapeutical areas in which the number of patients is large and the negotiated price, at least partly based on therapeutic added value, is high. However, patents are also an artificial barrier to competition, which prevents other firms from producing a similar drug, and discourages process innovation to produce it at the lowest cost. An alternative to patents would be innovation prizes (Geoffard 2020), in which financing authorities commit to pay a high lump-sum payment to the inventor of a socially desirable drug to buy out its patent; this allows ex post competition, reduces costs for health insurance, and requires an upfront investment which is a substitute to future profits paid during patent protection.
As stated above, some recent innovations, and others in the pipeline, have a very high production cost. Some gene therapies may cost more than €1 m for a single treatment, which has to be tailored to each patient. However, when they concern only a very small number of patients each year, even such sky-rocketing prices do not threaten health insurance budgets. Investing in such innovations is important to attract localisation of R&D units in Europe, as well as to reduce the delay patients experience before being able to access the treatment.
Innovation is not everything. Production also matters, and requires investment in production lines. This fact is highly visible for vaccines against COVID-19, for which limited production capacities reduce the speed at which populations could be vaccinated throughout the world. And though we do not know when a new virus will strike, we know it will happen again, some time in the future. However, we do not know its features, and of course we do not have treatments nor vaccines on the table for these future viruses. New technologies such as mRNA have shown their ability to offer a fast and efficient response to new viruses, and seem particularly powerful in a situation with a high uncertainty, as they can be adjusted to the specific characteristics of the still-to-come virus.
In that sense, setting up large production lines (which can be mobilised rapidly whenever a new pandemic hits the world) now is also an investment that could enable us, in the future, to respond much more rapidly and to avoid the health, economic, and social crises that we witnessed in 2020 and 2021. Investing in flexible, adjustable, vaccine production lines could be worth considering.
Finally, the COVID-19 crisis has also shown how the whole supply chain for certain pharmaceutical drugs can be very fragile, as it relies on a very small number of upstream producers of active ingredients, mostly located outside Europe. Relocating the production of some of these components in Europe could indeed be an answer to this fragility, but it will also require important investment.
8.5 Prevention
Preventing, at the individual or societal level, the occurrence of a future illness, or reducing its severity, is a textbook example of investment in health. As an old proverb attributed to Erasmus says, “Prevention is better than cure”. Is it really? The answer is a typical economist one: “It depends”. Some preventive actions, like vaccination, come at a small cost, and may produce high health benefits in the future. However, some other preventive actions do improve future health or reduce future mortality, but the cost per life saved, or per year in good health gained, is out of range with other, preventive or curative, interventions (Tengs et al. 1995).
Preventive care also typically represents a small share of total healthcare expenditure (Figure 4), and varies a lot across countries, ranging from 5.1% in the UK to less than 0.8% in Slovakia.
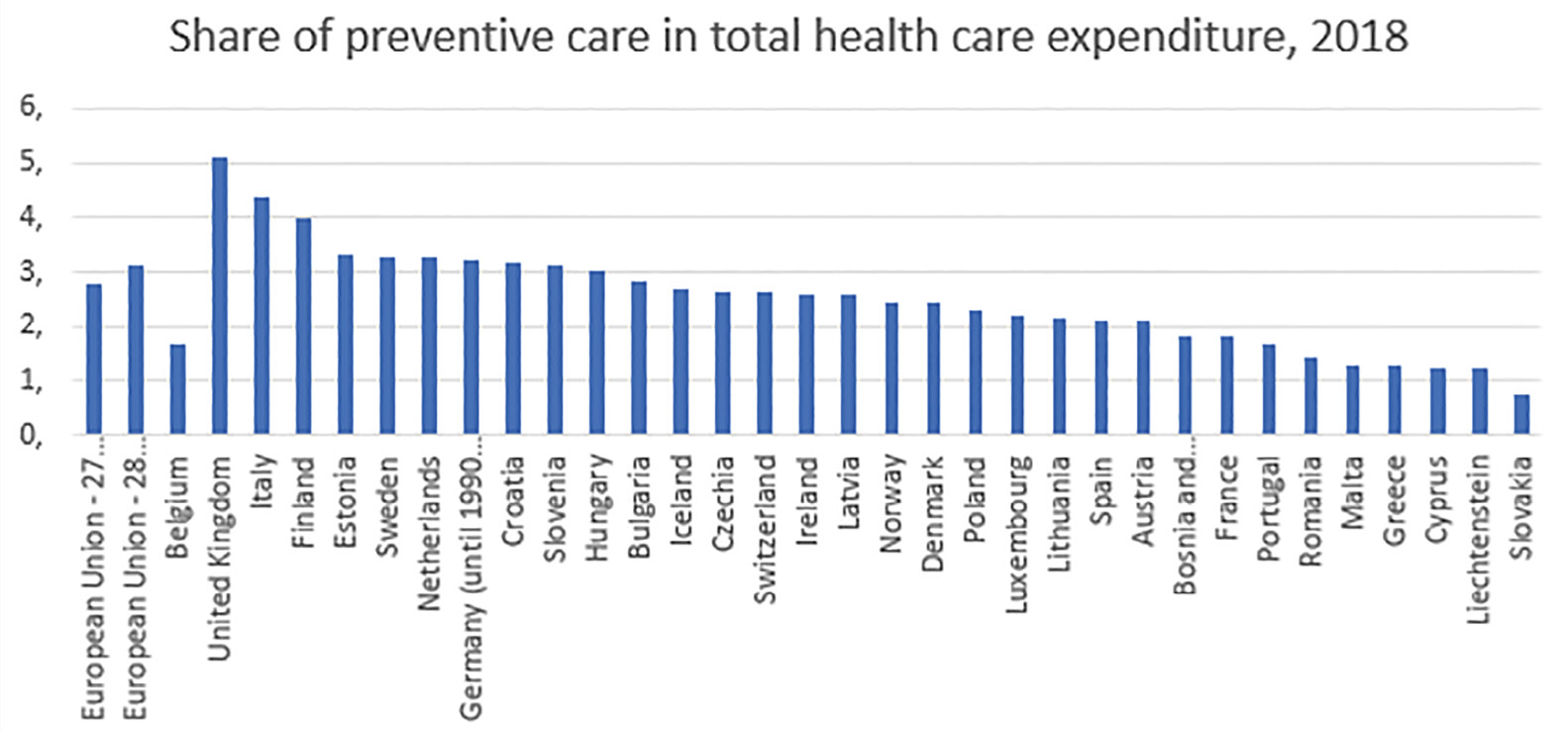
Fig. 4 Share of Preventive Care in Total Healthcare Expenditure, 2018.
Source of data: Eurostat, https://ec.europa.eu/eurostat/databrowser/view/HLTH_SHA11_HC__custom_423640/bookmark/table?lang=en&bookmarkId=5a8bfe63-5f2d-475c-b221-d7480f54fba3.
Notice that the average share of healthcare expenditure devoted to prevention dropped from 3.12% to 2.77% when the UK left the EU. This points out how much the UK National Health Service is rooted in prevention. Physicians, or more precisely group practices made up of several healthcare professionals, are partly financed according to their involvement in prevention. The health indicators in the UK are comparable to other countries of similar per capita GDP (e.g., same life expectancy at birth for men as in France), but the UK devotes a substantially lower share of GDP to healthcare expenditures (9.8% in 2019). In addition, whereas economic inequality is large in the UK, the association between socioeconomic status and health, at the individual level, seems weaker than in other comparable countries. In most countries, shifting from a healthcare system mostly centred on hospital care towards a more decentralised system, where general practice is the entry point into healthcare and tackles prevention as well as reduction of health inequalities, is an option to consider. Would such a shift require huge investment? Not necessarily, but such a reorganisation would be so disruptive to many healthcare professionals that it would surely need to be accompanied by important investment in organisation strategy, information systems, and training.
More generally, in the era of evidence-based medicine, prevention suffers from a disadvantage with respect to curative medicine: it is less often evaluated, impact evaluation being more difficult to assess due to the multiplicity of causes for any disease, the unknown duration before effects materialise, and the huge heterogeneity of situations. Better evidence on the costs and benefits of disease prevention across the board could yet be produced. Another similar investment in knowledge would also be welcome, to better understand the causal mechanisms underlying the strong socioeconomic inequalities witnessed in all countries.
To conclude on prevention, the ongoing COVID-19 crisis has shown a major weakness of health systems in Europe and elsewhere. Epidemiological surveillance failed to detect early diffusion of the virus in certain European countries or regions, at a time where it would have been possible to break, or at least to delay, the epidemic. This, also, needs to be strengthened in the future, if we want to be better prepared for the next pandemic.
8.6 Conclusion
The healthcare sector is, in essence, a very innovative industry in all its components. In conclusion, it should be reminded that if the years to come are associated with attempts to reduce public expenditure in order to repay the debt inherited from the COVID-19 crisis, such budget cuts should be contemplated with great prudence if they affect healthcare expenditure. In a sector where the main input is labour, budget cuts often lead to delayed or foregone capital investment, not because they are less efficient, but because they are easier to reduce.
However, demographic trends, digitalisation, and an increased role of prevention are the structural drivers of transformation in healthcare, and such changes will require important investment in the future.
References
European Commission (2014) Investments in Health: Policy Guide for the European Structural and Investment Funds 2014–2020, https://ec.europa.eu/health/sites/default/files/health_structural_funds/docs/esif_guide_en.pdf.
Geoffard, P. Y. (2020) Covid-19: Speeding up Vaccine Development, https://voxeu.org/article/accelerating-development-covid-19-vaccine.
Kremer, M., J.D. Levin, M. Christopher and C.M. Snyder (2020) Designing Advance Market Commitments for New Vaccines, NBER wp 28168, https://www.nber.org/papers/w28168.
OECD (2019) Health at a Glance 2019: OECD Indicators. Paris: OECD Publishing, https://doi.org/10.1787/4dd50c09-en.
Tengs, T. O., M.E. Adams, J.S. Pliskin, D.G. Safran, J.E. Siegel, M.C. Weinstein and J.D. Graham (1995) “Five-Hundred Life-Saving Interventions and Their Cost-Effectiveness”, Risk Analysis, 15(3): 369–90.
1 https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Healthcare_expenditure_statistics.
2 OECD (2020) Who Cares? Attracting and Retaining Care Workers for the Elderly https://www.oecd.org/health/who-cares-attracting-and-retaining-elderly-care-workers-92c0ef68-en.htm