
5. Ectogestative Technology and the Beginning of Life
© 2023 Lily Eva Frank, Julia Hermann et al, CC BY-NC 4.0 https://doi.org/10.11647/OBP.0366.05
How could ectogestative technology disrupt gender roles, parenting practices, and concepts such as ‘birth’, ‘body’, or ‘parent’? In this chapter, we situate this emerging technology in the context of the history of reproductive technologies and analyse the potential social and conceptual disruptions to which it could contribute. An ectogestative device, better known as ‘artificial womb’, enables the extra-uterine gestation of a human being, or mammal more generally. It is currently developed with the main goal of improving the survival chances of extremely premature neonates. We argue that the intended use of the technology in neonatal intensive care units, as an alternative to current incubators (’partial-ectogestation’), challenges concepts such as ‘birth’, ‘fetus’, and ‘neonate’, and has several ethico-legal implications. We moreover address a more futuristic scenario where the entire embryological and fetal development could happen within an artificial womb (’full-ectogestation’). Such a scenario reveals the disruption of gender roles, parenting practices, and concepts such as ‘mother’, ‘father’, and ‘parent’. Both full- and partial-ectogestation would have implications for engineering and design, law-making, ethics, and philosophical anthropology.
Fig. 5.1 Artificial womb. Credit: Menah Wellen
5.1 Introduction
The topic of reproduction touches on an inherent and central aspect of human existence. Humans across time and space have associated fertility with divine powers and have shrouded the beginning of life with mystical origins. In parallel, some of the key developments that have shaped reproductive medicine have increasingly sought to tame, probe, tinker, uncover, and control the mysteries of reproduction and the womb (Romanis et al., 2020).
Throughout the twentieth century, scientists and physicians portrayed the first incubators for early premature neonates as a means ‘to replace rather than enhance’ maternal2 connection (Horn, 2020). Similarly, ultrasound checks during pregnancy were introduced in 1956, and while they enable predictions of the sex of the fetus and screenings for any congenital abnormalities, ultrasound has also been weaponized as a personhood-deciding machine in the abortion debate. Ultrasound images enable the outside world to get a view into the womb, yet should not be seen as a mere window into the womb, as they present the first image of the fetus, as a single entity, distinct from its mother (Verbeek, 2008; Mills, 2014). According to Verbeek (2008), the fetus is thereby constituted both as a person and as a patient. In the 1960s, the contraceptive pill disrupted social norms by divorcing sex from reproduction for many women. The role of the maternal womb was once again challenged in 1978 when the first IVF baby Louise Brown saw the light, demonstrating that scientific prowess could overcome and control the wonders of conception beyond the womb. Current techniques enable researchers to culture embryos in vitro for longer than 14 days. Despite the so-called ‘14-day rule’, which is an international ethical standard that was first introduced in the UK by the Warnock Report (1984) and which forbids research on embryos past this point, the limit is increasingly being called into question (McCully, 2021). Consequently, with the track record of biomedicine, the advent of artificial wombs and the complete dissociation of reproduction from the maternal body might seem the next logical step of science’s triumph over human biology (Rifkin, 2002).
In this chapter, we situate ectogestative technology in the context of the history of reproductive technologies, and analyze some of the potential social and conceptual disruptions to which this emerging technology could contribute. But what is an ectogestative device (artificial womb)? Simply put, it is a device that enables the extra-uterine gestation of a human being, or mammal more generally.3 The first recorded mention of an artificial womb stems from the sixteenth-century writings of Swiss physician Paracelsus (Grafton, 1999). Four centuries later, British biologist J. B. S. Haldane revisited the topic of artificial wombs in a 1923 lecture. He coined the term ‘ectogenesis’ to describe the complete process of extra-uterine gestation of a human being from fertilization to birth. Stemming from the Greek words ‘ecto-’ and ‘genesis’ it literally reads as ‘outside development’. Haldane predicted ectogenesis would list amongst the most important discoveries of human history and propel radical social change such as emancipating women from the biological necessity of pregnancy for reproduction (Schwartz, 2019; Haldane, 1924). However, as with several major technological developments, artificial wombs gained traction through fiction like Aldous Huxley’s 1932 dystopian novel Brave New World and more recent feminist accounts, such as Helen Sedgwick’s The Growing Season (2017) and Rebecca Ann Smith’s Baby X (2016).
While film and literature may have the public dreaming about far future technologies, recent biomedical developments suggest that machine-mediated gestation no longer resides solely in the sphere of science fiction. Today, development at conception (with IVF techniques) and towards the late end of the gestation period (from ~24 weeks out of a typical pregnancy of 40 weeks, due to high-tech neonatal incubators) can already occur outside of the maternal body (Singer and Wells, 2006). As such, while full ectogenesis is still out of reach, partial-ectogestation, ‘the partial development of new mammals outside the maternal body, where normally this development happens inside’, is already a reality (Kingma and Finn, 2019: 356).
Notwithstanding the location, the kind of development that occurs ex utero is also an important aspect of research and controversy. The advances in neonatal intensive care now enable premature neonates to survive; however, for extremely premature neonates born under 28 weeks, chances of survival drop and the transition to independent life is often complicated by the immaturity of organs such as the lungs, guts, heart, and the brain (Lincetto & Banerjee, 2020). This often leads to lifelong physical and mental health complications (van der Hout-van der Jagt et al., 2022). The lack of improvement in extremely premature survival has indicated to many researchers that neonatal intensive care has reached a threshold of efficacy with ventilation-based life-support, and thus researchers have endeavored to develop alternative therapeutic means to improve survival. To this end, in 1997 at Juntendo University (Japan) Dr. Yoshinori Kuwabara and his team developed an extra-uterine fetal incubation system (EUFI) and were able to transfer fetal goats out of the doe’s womb and maintain them in fetal physiology submerged in a box with artificial amniotic fluid. Unfortunately, the goats were not able to survive the transition once removed from the device (Gelfand, 2006).
Twenty years later though, in 2017, a team at Philadelphia Children’s Hospital developed the ‘biobag’, a hermetically-sealed pouch that successfully enabled the transfer and gestation of fetal lambs to term (Partridge et al., 2017). A similar device, EVE or the ‘ex vivo uterine environment therapy’ was also successfully developed by an Australian-Japanese team (Usada et al., 2019). In both devices, the lambs float in artificial amniotic fluid and the umbilical cord is preserved and connected by a cannulation system to an external device, providing nutrients and oxygenating the blood, thus serving as placenta. In addition, the system is pumpless meaning the fetal heart alone powers the circuit, replicating in utero conditions and blood circulation (Partridge et al., 2017; Usada et al., 2019). In 2019, a multidisciplinary team of researchers at Eindhoven University of Technology (The Netherlands) set out to design and develop the PLS or ‘Perinatal Life Support System’ aimed at extremely preterm human neonates in the coming decades (CORDIS, 2019; Verweij et al., 2021).
As it stands, these devices are solely meant to serve as a therapeutic alternative to standard neonatal intensive care. Current researchers do not aim to push the limits of viability or carry out full-ectogestation. In the following sections, we argue that the intended use of the technology in neonatal intensive care units challenges concepts such as ‘birth’, ‘fetus’, and ‘neonate’, and has several ethico-legal implications. We moreover address a more futuristic scenario where the entire embryological and fetal development could happen within a technological device (’full-ectogestation’). Any claims related to full-ectogestation are highly speculative. Apart from the fact that we do not know whether it will ever be technically possible, we also do not know how safe it would be for the fetus, how it would affect parent-child bonding, how expensive it would be, who could afford it, and so forth. Given the fast pace of technological development and the human tendency to push things further, philosophers, designers and artists are creating and reflecting upon possible scenarios. The use of technomoral scenarios (see Boenink, Swierstra and Stemerding, 2010) to anticipate possible disruptions related to full-ectogestation can help to get a clearer idea of what is at stake when developing this technology and what would be (un)desirable. The scenario we address below (Section 5.3.2) reveals the potential disruption of gender roles, parenting practices, and concepts such as ‘mother’, ‘father’, and ‘parent’.
In our own research, we have, together with a speculative designer, organized stakeholder workshops, in which the discussion of technomoral scenarios was combined with prototyping activities. One of the issues addressed in relation to a technomoral scenario around partial-ectogestation was how parents could connect to the human being in the ectogestative device and whether the device should be portable, transparent, located in a hospital or at home.4 Both full- and partial-ectogestation have implications for engineering and design, law-making, ethics, and philosophical anthropology, to which we will return in the final section (Section 5.4).
5.2 Impacts and social disruptions
The development of ectogestative technology could usher in several impacts and social disruptions, divided here into three broad categories: 1) gender roles and the family, 2) moralization and de-moralization, and 3) medicalization. This section is divided into two parts, the first focusing on partial-ectogestation and the second on full-ectogestation. Although already partial-ectogestation challenges gender roles and the family to some extent, this is mainly the case for full-ectogestation, which is why we discuss this category only under full-ectogestation (Section 5.2.2).
5.2.1 Partial-ectogestation
Moralization and de-moralization
Ectogestative technology could contribute to the moralization of certain issues, and to the de-moralization of others. Moralization is the phenomenon by which something that was at one point considered to be a morally neutral choice, act or state of character changes into something that is evaluated from a moral perspective, within a particular society. De-moralization is the opposite process: what used to be considered morally right or wrong comes to be regarded as morally neutral. A classic example of moralization is the shift from smoking being seen merely as a matter of personal preference to a habit that is the object of social disgust and moral judgment, especially when one’s smoking impacts the health of others (second hand smoke) (see e.g. Eriksen, 2020). An example of de-moralization is the process in which, in some parts of the world, sexual preferences came to be seen as neither right or wrong.
The process of moralization is not in and of itself morally good or bad; this requires an independent evaluation. However, many of the decisions that pregnant people make are heavily moralized. The negative effects of alcohol on the developing fetus mounted and public awareness spread, starting in the 1970s. Since then, drinking alcohol during pregnancy has become increasingly moralized in many Western societies, particularly in the United States. Pregnant women who drink (or use drugs) are judged not only as doing something unhealthy, but as doing something morally wrong. Similar patterns surround consumption of certain foods, being overweight, opting for elective cesarean section instead of vaginal delivery, and, after birth, choosing formula or breastfeeding.
Considering the many ways in which the choices of pregnant women and new mothers/parents are moralized, it seems likely that the introduction of ectogestative technology could come with further moralization. As stated earlier, partial-ectogestation is intended to be used to mitigate the health impacts of being born prematurely. When a new medical intervention or technology comes into use, its very existence as an option changes the range of decisions with moral import that a patient can make. New options for care can be experienced as burdensome, forcing people to make medical decisions that would not have previously been available to them. For example, prenatal genetic testing gives pregnant people more information about the traits their fetus carries allowing them to choose to terminate their pregnancy (Verbeek, 2009). Other people may experience this new information and the new choices that it presents them with as liberating. The possibility of using ectogestative technology for fetuses that would otherwise be born prematurely and face risks of death and disability will mediate the choices that the prospective parents can make. These choices are likely to be seen as heavily morally laden. The phenomenon of the ‘technological imperative’ in health care may intensify these effects, although the influence of this effect will likely vary widely between different types of health care settings and national and cultural contexts (Koenig, 1988). The technological imperative has been observed by social scientists of medicine, who argue that once an advanced technology is introduced into medical care, physicians and hospitals feel a mandate to use them, regardless of whether or not they serve the patient’s interests (Koenig, 1988; Rothman, 1997; Hofmann, 2002).
Medicalization
Ectogestative technology can be expected to accelerate the process of medicalization of pregnancy and giving birth. Medicalization is the phenomenon by which a condition, behaviour, or physical/mental state changes from being a matter of choice or mere difference to being a matter which can be described, labeled, and potentially treated by doctors. Medicalization is not inherently positive or negative. Two classic examples illustrate this. The medicalization of certain mental health conditions like schizophrenia has shifted the way people understand those suffering from the condition away from seeing them as evil, possessed by spirits, or defective in character, to seeing them as people with a medical condition. This also comes with the possibility of researching and discovering treatments, medications, and therapies which may help to relieve the suffering and include patients in the community. Arguably, this form of medicalization, which moved certain mental maladies from being seen as personal or spiritual defects to psychological problems has on balance been a good thing for the well-being of these individuals (Conrad and Schneider, 1992). On the other hand, medicalization has been used to obfuscate injustices or recast human responses to their conditions as medical problems, e.g. drapetomania, the ‘mental illness’ that caused enslaved African people to tend to run away (Myers, 2014). In many places in the world, homosexuality is still labelled a disease.
Pregnancy and birth have been heavily medicalized in many WEIRD (Western, educated, industrialized, rich and democratic) countries and this medicalization has been subject to critiques, particularly by feminist thinkers (e.g. Rothman, 1991; Harley, 1993; Cahill, 2001; Beech and Phipps, 2008; Nisha, 2021), who are suspicious of the transfer of power and decision making surrounding pregnancy from pregnant women and their midwives to a patriarchal, technological, male-dominated medical establishment.5 The development of partial-ectogestation is likely to contribute to further medicalization of pregnancy and birth. Assuming that the chances for survival and a life without severe handicaps would increase significantly, it can be expected that pregnancies would be monitored even more closely than they are now and the numbers of extremely premature babies in neonatal intensive care units would rise. This of course also depends on the costs of the technology.
5.2.2 Full-ectogestation
Gender roles and the family
Ectogestative technology, particularly full-ectogestation, could cause disruptions to dominant gender roles in families and in parenting practices, which remain strong around the world despite women’s participation in the labor market. From a feminist perspective, such disruptions would be desirable. In many families, women still do the majority of child care and are assumed to have a special kind of bond with infants and children. As care ethicist Joan Tronto (1993: 103) points out, care is often ‘described and defined as a necessary relationship between two individuals, most often a mother and a child […] leading to a romanticization of mother and child, so that they become like a romantic couple in contemporary Western discourse’. If this special bond is partially constituted or justified by the fact that biological mothers ‘carried the baby’ inside their body for nine months of gestation, then full-ectogestation may challenge this assumption. A concern cited in the literature is that of a perceived threat to mother-child or maternal-fetal bonding that could be posed if the fetus spends some or all of its development in the ectogestative device instead of inside, or as part of, the maternal body (Landau 2007; de Bie et al., 2022; Lubetzky, 2020). Changes to the process of maternal-fetal bonding may challenge gender roles and the family because the nine months of pregnancy have historically been one of the purportedly scientific justifications for the special relationship between mother and infant (Creanley, 1981; Leifer, 1980). Thus, to the extent that this process is disrupted or perceived to be disrupted by ectogestative technology, gender roles in parenting may shift.
Maternal-fetal bonding (sometimes called attachment) can be defined as ‘an abstract concept, representing the affiliative relationship between a parent and a fetus, which is potentially present before pregnancy, is related to cognitive and emotional abilities to conceptualize another human being, and develops within an ecological system’ (Doan and Zimerman, 2008: 110). Concerns about the disruption of this process have to do with the long-term psycho-social development of the child, the trusting relationship between the parent and the child, and even impacts on fetal physiology (brain structure). The mechanisms of prenatal bonding and their impact on postnatal bonding are complex and mediated by a wide variety of factors, such as maternal stress and anxiety, as well as social support (Göbel et al., 2018). For example, Alhusen’s (2008) literature review on the topic identified multiple variables that have been hypothesized to impact maternal-fetal bonding and been empirically researched, such as demographic factors (e.g. maternal age), ‘perception of fetal movement’, presence of mood disorders in the mother, substance use during pregnancy, and previous pregnancy loss (Alhusen, 2008: 319).
There is mixed evidence that the use of technology can impact maternal-fetal bonding. For example, research by Ji et al. (2005) shows that pregnant women who were shown three-dimensional versus two-dimensional ultrasound images of their fetus showed greater signs of increased maternal-fetal bonding, such as being able to form a ‘mental picture’ of their baby, and were more likely to feel that they already ‘knew’ the baby when it was born.
Full-ectogestation could potentially open opportunities for fathers to have stronger bonds with their babies, freed from the expectation that they have a more distanced relationship with their child compared to the parent that gave birth. In homosexual or queer relationships, this may further equalize the parenting roles. It has to be noted though that there are no universal family structures or gender roles. There are significant cross-cultural differences in the structure of the family. The nuclear family, in which a male and female parent live together and raise children, is not a universal phenomenon. Nor is the structure in which the mother plays the role of main caregiver universal (Ruspini, 2015). We are here focusing on the possible disruptions to the Western paradigm, thereby acknowledging that the disruptive effects of this technology are likely to be different in other contexts. For instance, in more communal societies, the role of raising children is distributed among many people, including not only relatives but also neighbors and other inhabitants of the same community. However, it is usually women who play this role (see e.g. Edwards, 2000).6
Moralization and de-moralization
Further research would be needed to understand how the development of full-ectogestation may create instances of new moralization. People wishing to have a biological child may face social and moral pressure to use ectogestative technology. Although at this point, this is merely speculation, moral pressure could arise because it could seem to provide a safer and more controlled environment for fetal development than the maternal body. The fetus can be exposed to fewer risks and can be continuously monitored. On the other hand, the possibility of full-ectogestation could create the opposite kind of social and moral pressure. Choosing ‘natural’ pregnancy might be characterized as the more virtuous choice.7 Women who use ectogestative technology conversely might be painted as selfish, cold, or lazy. Within the workplace, opting for a ‘natural’ pregnancy over ectogestation may be viewed negatively from the perspective of productivity and ambition. Taking the needed parental leave to deliver and recover from pregnancy may be seen as selfish, afterall in many professions this time off puts additional burdens on co-workers to pick up the slack. Employers could thus demand that their employees work more. Hooton and Romanis (2022) have recently argued that the field of employment law will need to address ectogestation and that the reproductive rights of employees with respect to employers should not be ‘stratified’ or understood any differently depending on the bio-technological interventions that they use to reproduce.
One new area in which moralization may play a role and which has been extensively discussed in the emerging literature on the ethics of ectogestation is abortion. Induced abortion is defined in the medical literature as a procedure, either medical or surgical, which ends a pregnancy (Blackshaw and Rodger, 2019; Cohen, 2017; Räsänen, 2017). As Cohen explains, the possibility of ectogenesis (prima facie) removes the most morally and legally influential justification for a woman’s right to an abortion — bodily autonomy based on the presumption of gestational parenthood. If the termination of a pregnancy no longer necessarily involves the death of the embryo or fetus, the societal (and potentially conceptual) disruptions could involve changes in the meaning of abortion itself, changes in the moral and legal permissibility of abortion, and changes in the moral rights and responsibilities of genetic parents.
We can also envisage processes of de-moralization, e.g., regarding the behaviour of becoming mothers. If full-ectogestation were to become a reality and the mother’s behaviour ceased to have a direct effect on the development of the fetus, it would probably not be judged in moral terms anymore.
Medicalization
Full-ectogestation would allow for more and earlier medical interventions on the developing fetus. It may also allow for the environment to be optimized for a variety of growth and developmental factors, and for the fetal development and the environment to be constantly monitored to look for early signs of abnormalities, distress, or ways in which the environment could be improved. Ectogestation might also create opportunities for simple forms of human enhancement, for example, by allowing longer gestation times, which are associated with better cognitive capacities (Vollmer and Edmonds, 2019).
5.3 Conceptual disruption
Intricately related to the potential social impacts and disruptions just described, we can imagine several conceptual disruptions. Again we will start with disruptions related to partial-ectogestation and subsequently address disruptions that full-ectogestation might lead to. While already the advent of partial-ectogestation challenges concepts related to the beginning of life, body and personhood, full-ectogestation can be expected to disrupt concepts related to the family, gender, and parenthood. It should be noted that earlier reproductive technologies, as well as developments in medical science, also contributed to conceptual disruptions. Ectogestative technology is thus not unique in this respect, but it seems to exacerbate these processes of disruption.
5.3.1 Partial-ectogestation
Beginning of life
The advent of partial-ectogestation will challenge existing concepts and biological classifications around the beginning of life. Birth has historically stood for the detachment of the offspring from its mother’s womb and the beginning of independent life. However, partial-ectogestation will turn a coetaneous physical and physiological process into a fragmented one, consisting of two distinct events. The first event — ‘birth-by-location change’ — would happen when the fetus is separated from the maternal body and translocated to an ectogestative device. Because the device maintains fetal physiology ex utero, the second event, namely ‘birth-by-physiology change’ would only occur after extrication from the machine and successful transition to neonatal stage by breathing in oxygen from the air into the lungs and feeding through the mouth instead of the umbilical cord (Kingma and Finn, 2020).
The significance of birth is not limited to medical classification or social purposes, such as birthdays. Birth is also the moment at which some changes in the legal and moral standing of the infant occur. Before birth, in many legal systems, viability is the point at which the fetus gains the status of an individual with rights distinct from the pregnant person. In medical contexts, this means that physicians have responsibilities to the fetus as a patient distinct from the mother and may even conceive of the possibility of so-called ‘maternal-fetal conflicts’ occurring (Fasouliotis and Schenker, 2000). But birth itself also carries legal significance, for example, one standard means of determining whether neonaticide has occurred forensically is examining the lungs for evidence that the infant was ‘born alive’ or took its first breath (Phillips and Ong, 2018). In many places, parental responsibility and decision-making rights also shift legally after birth. While ‘inside’ the maternal body, medical care decisions about the fetus may be the responsibility of both parents, but are the right of the pregnant woman to make. After birth, if a second parent is present (usually genetic parent, in the male, cis-hetero case), he has an equal legal right to make medical decisions about the care of the newborn.
The socio-moral significance of birth can also be inferred from the complex ways in which people in many societies experience and react to the loss of life of the fetus (miscarriage) versus early infant death. Ectogestation complicates matters as experts will have to come together and decide which birth (birth-by-location change or birth-by-physiology change) should take normative precedence. This decision will have strong ethico-legal implications for the abortion debate, medical decision-making in obstetric care, and maternal-fetal conflicts.
Moreover, if a premature fetus is partially born and transferred to an ectogestative device, meaning born-by-location change but not yet born-by-physiology change, then the appropriate term to refer to the human offspring inside the device necessitates re-evaluation. Developing humans are categorized as fetuses from the eighth week of gestation (Cleveland Clinic, 2020). When a fetus leaves the womb, it becomes a neonate or newborn. An offspring born preterm in the neonatal intensive care unit is still considered a neonate, for it must shoulder the burden of its own life, albeit with some assistance. However, the offspring in the ectogestative device follows a different creative and formative process, and while ex utero, it functions ‘as if the neonate had never been born’ (Romanis, 2018: 753). Recent literature on the metaphysics of pregnancy has also argued, based on metabolic, immunological, and topological grounds, that fetuses are more than just babies gestating in their maternal host. They are a developing part of their pregnant mothers and only become separate individual entities post-birth (Kingma, 2019). Consequently, ectogestation and the specific developmental stage before birth-by-physiology change may require a new term to distinguish the ex utero gestating offspring from fetus and neonate. We will return to this point in Section 5.4.
Body and personhood
Ectogestative technology gives rise to a re-examination of anthropological concepts, a re-negotiation of what it means to be a human being or a person. The technology challenges our previous ideas of human being, body, and personhood. The boundaries between animate and inanimate, between nature and culture/technology, human and non-human, body and technology become blurred. How can we redraw these boundaries responsibly? Ectogestative technology is changing the understanding of the body. For example, it raises the question whether the ectogestative device is really completely separate from the human body or could be seen as an extension of it (Puzio, 2022: 291–346). Disability studies, for example, have argued that technology is perceived as part of the body by those who are existentially dependent on it (wheelchairs, pacemakers, implants, etc.) (Graham, 1999: 119; Thweatt, 2016: 152; 2018: 371). Whether ectogestative technology is considered as being part of the body can be relevant for legal issues, such as the protection of the mother and her decision about her own body. Moreover, like other technologies, such as prostheses, ectogestative technology can be seen as something different from a mere imitation or extension of the human body. It challenges our understanding of the concept of the ‘human body’ as something individual, natural, or purely biological and in contrast with that which is social, cultural, or technological.
Similar to obstetric ultrasound, ectogestative technology affects the concept of personhood. According to Verbeek’s analysis of ultrasound technology, it contributes to the constitution of the fetus both as a patient and as a person (Verbeek, 2008). Arguably, by not only making the fetus appear as a being that is distinct from its mother, but actually forming an environment in which it can exist and develop independently of its mother, ectogestative technology contributes to the constitution of the fetus as a person (and patient) in an even stronger sense. This challenges the concept of personhood: who and what should count as a person?
5.3.2 Full-ectogestation
Parenthood
A cluster of concepts that is likely to be affected by full-ectogestation in particular is mother-father-parent-family-gender. Here we focus on the concept ‘mother’, while emphasizing that other concepts in the cluster are also affected. The concept of mother can be analyzed as having at least three different dimensions: genetic, gestational, and social mother (see Ber, 2000). Usually, people conceive of mothers as being mothers along all three dimensions. The three dimensions can come apart, however (see Fig. 5.2). A woman who has adopted a child is the child’s social mother, but not its genetic or gestational mother. A woman who has made use of surrogacy is the child’s genetic and social mother, but not its gestational mother. She could also be just the social mother, in case she made use of egg donation (see Fig. 5.2 for the different possible combinations). It should also be noted that social motherhood can be shared. The differentiations depicted in the table below are to a large extent due to the development of reproductive technologies, such as egg donation and IVF. The table contains three types of women who are mothers, though not gestational mothers: adoptive mothers or foster mothers, women who used surrogacy, and egg donors. This shows that also in the absence of the availability of full-ectogestation, becoming a mother without gestating a child is possible. Nevertheless, this technology poses a challenge to the concept of mother, by potentially creating the possibility for having a child without there being any gestational mother at all.
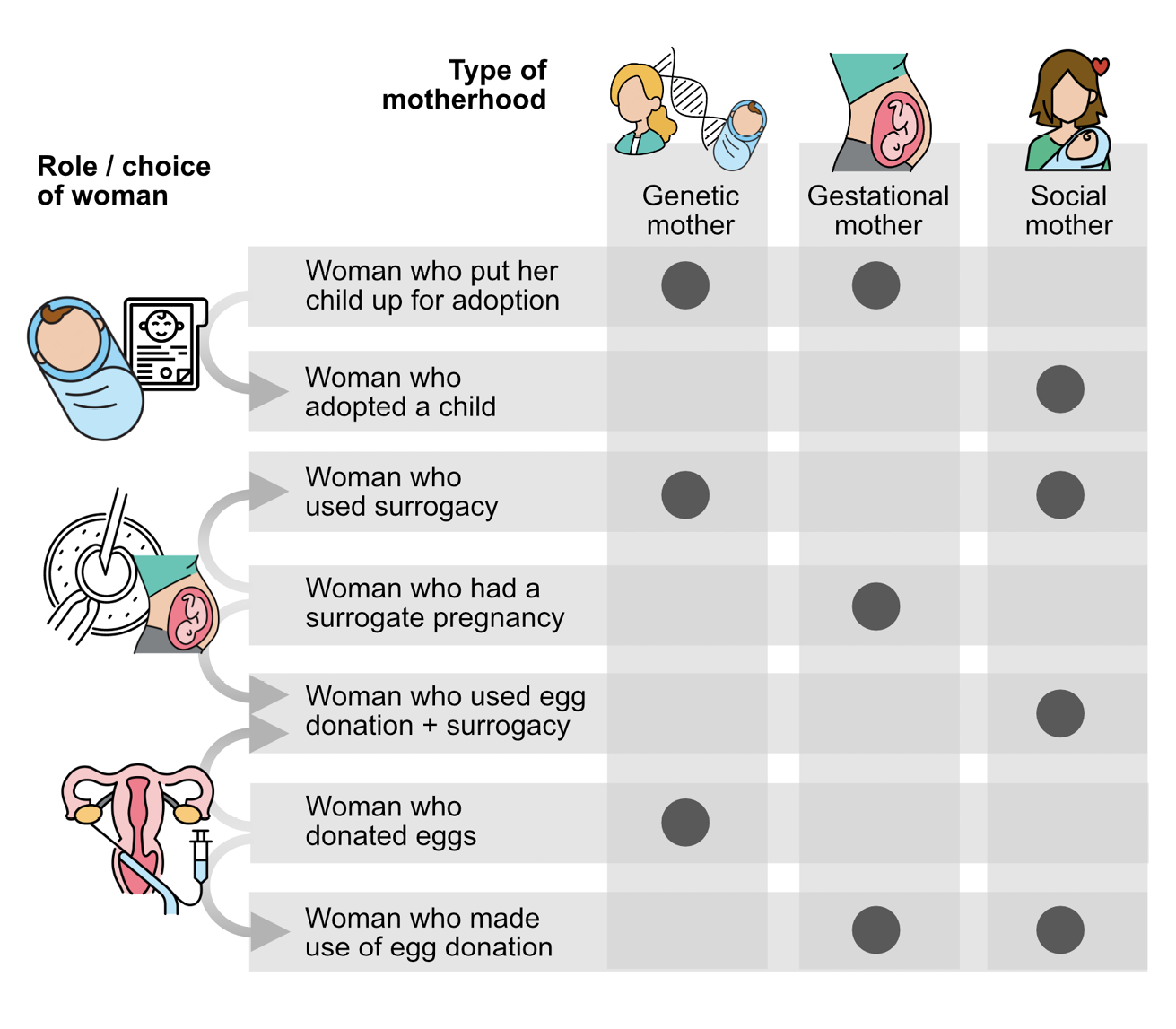
Fig. 5.2 Different types of motherhood. Credit: Ilse Oosterlaken
If the possibility of full-ectogestation were to become reality, there could be children who had only genetic and social mothers but no gestational mothers (see Jacobs, 2023). We can imagine a group of people raising a child together, where some of them might be the child’s genetic parents, while none of them is a gestational mother. In such a scenario, the question arises as to what makes a parent a mother as opposed to a father. If we think of a non-binary person being one of the parents of the child, is that person a mother or a father? While on our current understanding of motherhood, only female persons can be mothers, this scenario raises the question as to why being female should be a necessary condition for being a mother. The scenario invites speculation about whether we would still need the concept ‘mother’ at all or could replace both ‘mother’ or ‘father’ by ‘parent’.8
As mentioned above, full-ectogestation would also affect related concepts, such as ‘gender’ and ‘family’. The possible social disruptions discussed in the previous section (disruptions of family structures and gender roles) arguably also involve conceptual disruptions. For instance, by changing parenting practices and family constellations, the technology might have the potential to disrupt the Western concept of the nuclear family. In addition, the disruption of traditional gender roles affects the concept of gender, which is partly constituted by these roles.
5.4 Looking ahead
The further development of ectogestative technology has implications for engineering and design, law-making,9 ethics, and philosophical anthropology. Anticipating how the advent of ectogestation may disrupt various aspects of society and our notion of the beginning of life can be of use to designers, engineers, and ethicists alike in the research and implementation process. As mentioned above, concepts such as ‘birth’, ‘fetus’ and ‘neonate’ will need to be reevaluated. Partial-ectogestation in particular may introduce a novel development stage between fetus and neonate, which requires new terminology. To this end, several terms have begun to circulate in the literature, including ‘gestateling’ (Romanis, 2018), ‘fetonate’ (De Bie et al., 2022), and ‘perinate’ (Van der Hout-van der Jagt et al., 2022).
The disruption of birth occasioned both by practically fragmenting the process and conceptually clouding the distinction between fetus and neonate will have implications for ethics, law-making, and even the design of ectogestative devices. Birth is often used to demarcate the point in human development at which full legal personhood is assigned (Mills, 2014; Romanis, 2019). If birth-by-location change is granted the normative significance of birth as traditionally understood, then the ectogestative device will appear more similar to an incubator, harboring a neonate in a liquid environment. This implies that the moment at which full legal and moral status is attributed could remain as it is, namely after delivery from the maternal womb — thus topology wins. However, if birth-by-physiology change is attributed more significance, then the ectogestative device will be more akin to a device that simulates gestation in the maternal womb. Consequently, the gestating human in the device would be closer to a fetus than to a neonate and might only qualify for partial legal and moral status.
Beyond usability, the design of a technology can also be rooted in values that will guide usage and perpetuate encoded norms (Friedman et al., 2002). Thus, design requirements of an ectogestative device should reflect values and norms that we wish to abide by. These values will be informed by how we ontologically make sense of the technology and how it mediates our notion of the human being inside the device. For example, if it is perceived as being similar to a fetus, design priorities will likely lean towards mimicking womb-like conditions. However, if it is perceived as a neonate (but with fetal physiology as described by the US EXTEND team in De Bie et al., 2022), then extra consideration could be given to building a see-through device, making it portable, and allowing for as much contact as possible, as expected from current incubators. Moreover, if the human being in the device is conceptualized as something other than a fetus or neonate, and rather as a novel stage in human development, then design requirements will also need to be carefully assessed to be in accord with the law, ethics, and social mores.
When analyzing the social disruption brought about by a technology, it is also imperative to acknowledge how the technology is situated in the socio-material environment, as this will shape how it is appropriated. Reproductive technologies have often been lauded as progressive and liberating for many women, however, there has also been an increasing trend in biomedicine to medicalise reproduction, pregnancy, and the maternal body. For example, ultrasounds are disruptive for they can act as ‘moral speculum’. Beyond ascertaining the life of a fetus, they can serve as ‘personhood-deciding machines’ and become a medium for some women to choose for or against a termination of their pregnancy (Mills, 2014). With partial-ectogestation, while the impetus is on saving the extremely premature, we cannot risk effacing pregnant women both from their role in gestation and from stakeholder considerations in the research and design process. After all, it is through their body that we must first go to access the fetus. In addition, regarding full-ectogestation, it has to be kept in mind that the technology would use a lot of energy and there would be the need to justify why limited resources should be used for a device the function of which can, under normal circumstances, also be fulfilled by a female body. Consequently, for both partial and full-ectogestation it is imperative to think about how and where this technology will be situated, and to anticipate its misuse, so it is not introduced to exacerbate current injustices.
Our reflections with stakeholders on a scenario around partial-ectogestation revealed concerns about how to connect with the human being developing ex utero and a dissensus regarding whether the ectogestative device should mimic the maternal womb as much as possible or rather be designed differently, possibly improving upon the natural womb. Our reflections and workshop on more speculative scenarios around full-ectogestation showed that such scenarios seem to make room for an upgrading of fathers, overcoming traditional understandings of the roles and tasks of mothers, a more equal division of care labour and responsibility, and more possibilities for members of the LGBTQ+ community to become parents. They also supported worries about the potential negative effects on parent-child bonding and the physical and mental development of the human being developing ex utero. Given these worries as well those mentioned above concerning market driven pressures on women’s choices, one could conclude that an upgrading of fathers etc. should be promoted by other means than full-ectogestation, which is ultimately not desirable. Imagining possible futures with full-ectogestation would then be seen as helping us envision more vividly and forcefully the possibility and desirability of certain changes or disruptions, which we could then try to achieve by other means.
It is, moreover, important to include intercultural voices in the development of ectogestative technology. Attitudes towards the technology and the way it is dealt with will strongly depend on cultural factors and vary greatly according to cultural background. This makes interculturally sensitive development and handling of ectogestative technologies necessary. When it comes to questions of life and its beginning, religions play an important role. Despite the loss of importance of religions in many Western societies, these beliefs have strongly shaped the value systems of these societies, including the understanding of nature, creation, and human beings. As many cultural and religious traditions and rituals are associated with birth, it is likely that with ectogestative technology such rituals will undergo transformation and new rituals will emerge.
Since, as mentioned above, technologies can change our understanding of the human being and the body, they spur novel anthropological reflection. Technologies transport human understandings/conceptions of the human being. Therefore, it is important to critically examine which human understandings and discriminations are transported in technologies. Which patriarchal, sexist, racist, and heteronormative structures are taken over unnoticed in the design of ectogestative devices?
Anthropology is increasingly turning away from essentialist notions of a supposed ‘human nature’ towards a non-essentialist, dynamic, and fluid understanding of human identity. Assuming that the understanding of the human being is always in a state of flux and is not a constant or essence that transcends time, space, and culture makes it possible to think of it as open to (also technological) change. In particular, movements of thought such as New Materialism and Critical Posthumanism, which have been strongly influenced by Donna Haraway’s thinking, are striving to break down old anthropological concepts and dichotomies (of inanimate-animate, human-animal, human-machine, nature-culture/technology, woman-man). Haraway coined the ontological, epistemological, and political figure of the cyborg, which as ‘a cybernetic organism, a hybrid of machine and organism’ (Haraway, 2004: 7) has a hybrid, fluid, and dynamic identity. The cyborg is neither unequivocally human, nor animal nor machine, thus refusing any categorization and classification, and therefore has a ‘subversive potential … to resist any re-ontologization of the human’ (Ruf, 2001: 286; see also Chapter 3). There is no pre-existing ‘human nature’, but rather being human is produced in relationship and interaction with non-human entities (e.g., technologies or animals). Contemporary anthropology re-locates the position of the human being, valorizes non-human entities, and criticizes anthropocentrism. Critical Posthumanism and New Materialism reflect anew on concepts such as the human, the body, life, nature, matter, etc. They draw attention to the fact that technologies such as ectogestative technology blur the boundaries between animate-inanimate, human-animal, human-machine, nature-culture/technology, woman-man, question these boundaries and want to redraw them responsibly. In doing so, they draw attention to discrimination in these boundary drawing processes and encourage intercultural, anti-racist, and inclusive approaches. They also ask who determines which boundaries are drawn and advocate for the diversity of bodies and genders.
Further listening and watching
Readers who would like to learn more about ectogestative technology as a socially disruptive technology might be interested in listening to the following interviews and a related episode of the ESDiT podcast (https://anchor.fm/esdit):
Julia Hermann, Interview about the ethics of socially disruptive technologies for the Australian radio program Radical Philosophy, 3CR Community Radio, 22 January 2022: https://www.3cr.org.au/radicalphilosophy/episode-202201221330/ethics-socially-disruptive-technologies-dr-julia-hermann
Julia Hermann on ‘Ectogestative technology’, Focus, NPO Radio 1, 7 May 2021:
https://www.nporadio1.nl/podcasts/dekennisvannu/1375886-zwanger-of-een-kind-uit-een- kunst-baarmoeder
Julia Hermann on ‘The artificial womb’: https://www.esdit.nl/2021/esdit-podcast-julia-hermann-on-the-artificial-womb/
References
Alhusen, Jeanne L. 2008. ‘A literature update on maternal-fetal attachment’, Journal of Obstetric, Gynecologic & Neonatal Nursing, 37(3), 315–28, https://doi.org/10.1111/j.1552-6909.2008.00241.x
Beech, Beverley A. Lawrence, and Belinda Phipps. 2008. ‘Normal birth: women’s stories’, in Normal Childbirth: Evidence and Debate, ed. by Soo Downe (Elsevier, 2008, second edition), 67–81
Ber, Rosalie. 2000. ‘Ethical issues in gestational surrogacy’, Theoretical Medicine and Bioethics, 21, 153–69, https://doi.org/10.1023/A:1009956218800
Boenink, Marianne, Swierstra, Tsjalling, and Stemerding, Dirk. 2010. ‘Anticipating the interaction between technology and morality: A scenario study of experimenting with humans in bionanotechnology’, Studies in Ethics, Law, and Technology, 4(2). https://doi.org/10.2202/1941-6008.1098
Cahill, Heather A. 2001. ‘Male appropriation and medicalization of childbirth: An historical analysis’, Journal of Advanced Nursing, 33(3), 334–42, https://doi.org/10.1046/j.1365-2648.2001.01669.x
Cleveland Clinic. 2020. ‘Fetal development: Month-by-month stages of pregnancy’, Cleveland Clinic, https://my.clevelandclinic.org/health/articles/7247-fetal-development-stages-of-growth
Conrad, Peter, and Joseph W. Schneider. 1992. Deviance and Medicalization: From Badness to Sickness. (Temple University Press)
CORDIS European Commission. 2019. ‘Brave new world? Artificial womb prototype offering hope for premature babies’, CORDIS EU Research Results, https://cordis.europa.eu/article/id/411541-brave-new-world-artificial-womb-prototype-offering-hope-for-premature-babies
Cranley, Mecca S. 1981. ‘Development of a tool for the measurement of maternal attachment during pregnancy’, Nursing Research 30(5), pp. 281–84, https://doi.org/10.1097/00006199-198109000-00008
De Bie, Felix, Sarah Kim, Sourav Bose, Pamela Nathanson, Emily Partridge, Alan Flake, and Chris Feudtner. 2022. ‘Ethics considerations regarding artificial womb technology for the fetonate’, The American Journal of Bioethics, 1–12, https://doi.org/10.1080/15265161.2022.2048738
Doan, Helen, and Anona Zimerman. 2008. ‘Prenatal attachment: A developmental model’, International Journal of Prenatal and Perinatal Psychology and Medicine, 20(1–2), 20–28
Edwards, Arlene E. 2000. ‘Community mothering: The relationship between mothering and the community work of Black women’, Journal of the Association for Research on Mothering, 2(2), 87–100
Fasouliotis, Sozos, and Joseph Schenker. 2000. ‘Maternal–fetal conflict’, European Journal of Obstetrics & Gynecology and Reproductive Biology, 89(1): 101–7, https://doi.org/10.1016/S0301-2115(99)00166-9
Friedman, Batya, Peter H. Kahn, and Alan Borning. 2002. ‘Value sensitive design: Theory and methods’, University of Washington Technical Report, 2–12
Gelfand, Scott. 2006. ‘Introduction’, in Ectogenesis: Artificial Womb Technology and the Future of Human Reproduction, ed. by Scott Gelfand and John Shook (Amsterdam; New York, NY: Brill/Rodopi)
Göbel, Ariane, Lydia Yao Stuhrmann, Susanne Harder, Michael Schulte-Markwort, and Susanne Mudra. 2018. ‘The association between maternal-fetal bonding and prenatal anxiety: An explanatory analysis and systematic review’, Journal of Affective Disorders, 239: 313–27, https://doi.org/10.1016/j.jad.2018.07.024
Grafton, Anthony. 1999. Natural Particulars: Nature and the Disciplines in Renaissance Europe (Boston: MIT Press)
Graham, Elaine. 1999. ‘Words made flesh: Women, embodiment and practical theology’, Feminist Theology, 7(21): 109–21, https://doi.org/10.1177/096673509900002108
Haldane, John. 1924. Daedalus or Science and the Future (New York: Dutton), https://www.gutenberg.org/files/70955/70955-h/70955-h.htm
Haraway, Donna. 2004. ‘A manifesto for cyborgs: Science, technology, and social feminism in the 1980s’, in The Haraway Reader, ed. by Donna Haraway (New York: Routledge), 7–45 (Original work published in 1985)
Haslanger, Sally. 2014. ‘Social meaning and philosophical method’, Proceedings and Addresses of the American Philosophical Association 88: 16–37
Hofmann, Bjørn. 2002. ‘Is there a technological imperative in health care?’, International Journal of Technology Assessment in Health Care, 18(3): 675–89, https://doi.org/10.1017/S0266462302000491
Horn, Claire. 2020. ‘The history of the incubator makes a sideshow of mothering’, PSYCHE, https://psyche.co/ideas/the-history-of-the-incubator-makes-a-sideshow-of-mothering
Hooton, Victoria, and Romanis, Elizabeth C. 2022. ‘Artificial womb technology, pregnancy, and EU employment rights’, Journal of Law and the Biosciences, 9(1), lsac009, https://doi.org/10.1093/jlb/lsac009
Ji, Eun-Kyung, Dolores Pretorius, Ruth Newton, K. Uyan, Andrew D. Hull, Kathryn Hollenbach, and Thomas R. Nelson. 2005. ‘Effects of ultrasound on maternal‐fetal bonding: A comparison of two‐and three‐dimensional imaging’, Ultrasound in Obstetrics and Gynecology: The Official Journal of the International Society of Ultrasound in Obstetrics and Gynecology, 25(5): 473–77, https://doi.org/10.1002/uog.1896
Kingma, Elselijn. 2019. ‘Were you a part of your mother?’, Mind, 128(511): 609–46, https://doi.org/10.1093/mind/fzy087
Kingma, Elselijn, and Suki Finn. 2020. ‘Neonatal incubator or artificial womb? Distinguishing ectogestation and ectogenesis using the metaphysics of pregnancy’, Bioethics, 34(4): 354–63, https://doi.org/10.1111/bioe.12717
Koenig, Barbara. 1988. ‘The technological imperative in medical practice: The social creation of a “routine” treatment’, in Biomedicine Examined, ed. by Margaret Lock and Deborah Gordon (Dordrecht: Springer), 465–96, https://doi.org/10.1007/978-94-009-2725-4_18
Landau, Ruth. 2007. ‘Artificial womb versus natural birth: An exploratory study of women’s views’, Journal of Reproductive and Infant Psychology, 25(1), 4–17, https://doi.org/10.1080/02646830601117118
Leifer, Myra. 1980. Psychological Effects of Motherhood: A Study of First Pregnancy (New York: Praeger)
Lincetto, Omella, and Banerjee, Anshu 2020. ‘World prematurity day: Improving survival and quality of life for millions of babies born preterm around the world’, American Journal of Physiology-Lung Cellular and Molecular Physiology, 319(5), L871-L874, https://doi.org/10.1152/ajplung.00479.2020
Lubetzky, Ofra. 2020. ‘The maternal-fetus relationship in the uterus: Essential for wellbeing through life’, Journal of Prenatal & Perinatal Psychology & Health, 34(6)
McCully, Sophia. 2021. ‘The time has come to extend the 14-day limit’, Journal of Medical Ethics, 47(12): e66, https://doi.org/10.1136/medethics-2020-106406
Mills, Catherine. 2014. ‘Making fetal persons: Fetal homicide, ultrasound, and the normative significance of birth’, Philosophia, 4(1): 88–107, https://doi.org/10.26180/5f3f817b0a0c5
Myers II, B. E. 2014. ‘“Drapetomania” Rebellion, defiance and free Black insanity’, in the Antebellum United States (Los Angeles: University of California)
Nisha, Zairu. 2021. ‘Technicization of “birth” and “mothering”: Bioethical debates from feminist perspectives’, Asian Bioethics Review, 13, 133–48, https://doi.org/10.1007/s41649-021-00169-z
Partridge, Emily, Marcus Davey, Matthew Hornick, Patrick McGovern, Ali Mejaddam, Jesse Vrecenak, Carmen Mesas-Burgos, Aliza Olive, Robert Caskey, Theodore Weiland, Jiancheng Han, Alexander Schupper, James Connelly, Kevin Dysart, Jack Rychik, Holly Hedrick, William Peranteau, and Alan Flake. 2017. ‘An extra-uterine system to physiologically support the extreme premature lamb’, Nature Communications, 8(1): 15112, https://doi.org/10.1038/ncomms15112
Perrot, Adeline, and Ruth Horn. 2022. ‘The ethical landscape (s) of non-invasive prenatal testing in England, France and Germany: Findings from a comparative literature review’, European Journal of Human Genetics, 30(6): 676–81, https://doi.org/10.1038/s41431-021-00970-2
Phillips, Bianca, and Beng Beng Ong. 2018. ‘“Was the infant born alive?” A review of postmortem techniques used to determine live birth in cases of suspected neonaticide’, Academic Forensic Pathology, 8(4): 874–93, https://doi.org/10.1177/1925362118821476
Puzio, Anna. 2022. Über-Menschen. Philosophische Auseinandersetzung mit der Anthropologie des Transhumanismus (Bielefeld: transcript Verlag), https://doi.org/10.14361/9783839463055
Rifkin, Jeremy. 2002. ‘The end of pregnancy’, The Guardian, https://www.theguardian.com/world/2002/jan/17/gender.medicalscience
Rohwer, Yasha, and Emma Marris. 2018. ‘An analysis of potential ethical justifications for mammoth de-extinction and a call for empirical research’, Ethics, Policy & Environment, 21(1): 127–42, https://doi.org/10.1080/21550085.2018.1448043
Romanis, Elizabeth C. 2018. ‘Artificial womb technology and the frontiers of human reproduction: Conceptual differences and potential implications’, Journal of Medical Ethics, 44(11): 751–55, https://doi.org/10.1136/medethics-2018-104910
Romanis, Elizabeth. 2019. ‘Artificial womb technology and the significance of birth: Why gestatelings are not newborns (or fetuses)’, Journal of Medical Ethics, 45(11): 728–31, http://doi.org/10.1136/medethics-2019-105495
Romanis, Elizabeth, Dunja Begović, Margot Brazier, and Alexandra Katherine Mullock. 2020. ‘Reviewing the womb’, Journal of Medical Ethics, 47(12): 820–29, https://doi.org/10.1136/medethics-2020-106160
Rothman, Barbara Katz. 1991. In Labor: Women and Power in the Birthplace. (New York: W. W. Norton & Co)
Rothman, David. 1997. Beginnings Count: The Technological Imperative in American Health Care (New York; Oxford: Oxford University Press)
Ruf, Simon. 2001. ‘Über-Menschen. Elemente einer genealogie des cyborgs’, in Mediale Anatomien. Menschenbilder als Medienprojektionen (Kultur- und Medientheorie), ed. by Annette Keck and Nicolas Pethes (Bielefeld: transcript), 267–86, https://doi.org/10.14361/9783839400760-015
Ruspini, Elisabetta. 2015. Diversity in Family Life: Gender, Relationships and Social Change (Bristol: Policy Press)
Schwartz, Oscar. 2019. ‘On the history of the artificial womb’, JSTOR Daily, https://daily.jstor.org/on-the-history-of-the-artificial-womb/
Singer, Peter, and Deaene Wells. 2006. ‘Ectogenesis’, in Ectogenesis, ed. by Scott Gelfand and John Shook (Amsterdam; New York: Rodopi), 9–25, https://doi.org/10.1163/9789401203456_005
Sullivan, Lawrence, and Nancy Liu-Sullivan. 2021. Historical Dictionary of Chinese Culture (London: Rowman & Littlefield Publishers)
Thweatt, Jeanine. 2016. Cyborg Selves. A Theological Anthropology of the Posthuman (London: Routledge), https://doi.org/10.4324/9781315575728
——. 2018. ‘Cyborg-Christus: Transhumanismus und die Heiligkeit des Körpers’, in Designobjekt Mensch. Die Agenda des Transhumanismus auf dem Prüfstand, ed. by Benedikt Göcke and Frank Meier-Hamidi (Freiburg: Herder), 363–76
Tong-Hyun, Kim. (2023 29 June). “South Koreans grow younger overnight as the country changes how it counts people’s ages.” https://apnews.com/article/south-korea-age-counting-law-a38a4a6b47c6864bd13433fdac071cec
Tronto, Joan. 1993. Moral Boundaries: A Political Argument for an Ethics of Care (New York; London: Routledge)
Usuda, Haruo, Shimpei Watanabe, Masatoshi Saito, Shinichi Sato, Gabrielle C. Musk, Erin Fee, Sean Carter, Yusaku Kumagai, Tsukasa Takahashi, Shinichi Kawamura, Takushi Hanita, Shigeo Kure, Nobuo Yaegashi, John P. Newnham, and Matthew W. Kemp. 2019. ‘Successful use of an artificial placenta to support extremely preterm ovine fetuses at the border of viability’, American Journal of Obstetrics and Gynecology, 221(1): 69.e1–69.e17. https://doi.org/10.1016/j.ajog.2019.03.001
Van der Hout-van der Jagt, Beatrijs, Joanne Verweij, Peter Andriessen, Willem de Boode, Arend Bos, Frank Delbressine, Alex Eggink, Jan Jaap Erwich, Loe Feijs, Floris Groenendaal, Boris Kramer, Titia Lely Rachel Loop, Franziska Neukamp, Wes Onland, Martijn Oudijk, Arjan te Pas, Irwin Reiss, Mark Schoberer, Ralph Scholten, Marc Spaanderman, Myrthe van der Ven, Marijn Vermeulen, Frans van de Vosse, and Guid Oei. 2022. ‘Interprofessional consensus regarding design requirements for liquid-based Perinatal Life Support (PLS) technology’, Frontiers in Pediatrics, 9: 1601, https://doi.org/10.3389/fped.2021.793531
Verbeek, Peter-Paul. 2008. ‘Obstetric ultrasound and the technological mediation of morality: A postphenomenological analysis’, Human Studies, 31(1): 11–26, https://doi.org/10.1007/s10746-007-9079-0
——. 2009. ‘The moral relevance of technological artifacts’, in Evaluating New Technologies (Dordrecht: Springer), 63–77, https://doi.org/10.1007/978-90-481-2229-5_6
Verweij, Joanne, Lien De Proost, Judith van Laar, Lily Frank, Sylvia Obermann-Borstn, Marijn Vermeulen, Sophie van Baalen, Beatrijs van der Hout-van der Jagt, and Elselijn Kingma. 2021. ‘Ethical development of artificial amniotic sac and placenta technology: A roadmap’, Frontiers in Pediatrics, 9: 793308, https://doi.org/10.3389/fped.2021.793308
Vollmer, Brigitte, and Caroline Edmonds. 2019. ‘School age neurological and cognitive outcomes of fetal growth retardation or small for gestational age birth weight’, Frontiers in Endocrinology, 10: 186, https://doi.org/10.3389/fendo.2019.00186
1 All authors contributed original text to this chapter, commented on parts written by others and approved the final version. LEF and JH are the lead authors of this chapter. They coordinated the writing process and did the final editing. LEF wrote the first version of Section 5.2 and contributed to Section 5.3.2. JH wrote the first version of Section 5.3.2 and contributed to all other sections. LK wrote the first version of the introduction. LK and AP together wrote the first version of Section 5.3.1 and Section 5.4.
2 Throughout this chapter we use maternal/mother/motherhood/pregnant woman but recognize that transgender men and nonbinary people can also become pregnant and give birth. Using the ‘traditional’ terminology in this chapter highlights some of the more striking disruptions that this technology could usher in, including gender roles, family structure, and understanding of gender identity.
3 Our focus in this chapter is on the development of ectogestative technologies for human beings, but a note on its potential use for animals is in place. There are, for instance, efforts being made to develop an artificial womb that can be of use in the endeavor to bring back the extinct mammoth (’de-extinction’) (see e.g. Rohwer and Marris, 2018). It should also be noted that one of the ethical issues raised by the development of ectogestative technology for human beings is the use of animals in the research process. We thank Bernice Bovenkerk for drawing our attention to these points.
4 We collaborated with speculative designer Lisa Mandemaker in a project funded by ESDiT and DesignLab Twente. The following people participated in this collaborative research and design project: Patricia de Vries, Lily Eva Frank, Margoth González Woge, Naomi Jacobs, Julia Hermann, Llona Kavege, Lisa Mandemaker, Sabine Wildevuur, and Cristina Zaga.
5 Of course this is a major simplification, given that, for example, there are significant differences between countries in the European Union and the UK. C.f. Perrot and Horn (2022).
6 Current research on ectogestative technology takes place primarily in the United States (Partridge et al., 2017), Europe (Verweij, 2022), Australia (Miura et al., 2015), and Japan (IToH, 2010). There is to our knowledge no philosophical or ethical literature available from the Japanese context, which is why we focus on potential disruptions to the Western paradigm.
7 We use quotation marks here to signal that the term ‘natural’ is problematic. Given the role that technology has come to play in this context (think of ultrasound, prenatal diagnostics, IVF, pre implementation diagnostics, c-sections, etc.), we can ask ourselves how ‘natural’ a normal pregnancy actually is.
8 For a problematization of definitions of ‘mother’ and the categorization of people as mothers (instead of parents) see Haslanger (2014: 30f).
9 Legal and social conventions around birth: ectogestative technology can be expected to affect the conventions that we find in different cultures. For instance, legal and social conventions surrounding the date of birth differ culturally and have varied over time. For example, in Chinese culture, a baby’s first birthday occurs on the day they are born: they are already one year old. Whereas in western culture a baby’s first birthday occurs a year after they are born (Sullivan and Liu-Sullivan, 2021). In 2023 South Korea’s government officially changed the way citizen’s ages are calculated, shifting from infants being designated one year old at birth and two years old on January 1 of the first year of life, to a system which marks ages with the passing of birth days (Tong-Hyung, 2023). In Bhutan, traditionally, birthdays are not routinely celebrated and the date of one’s birth is not something one necessarily even knows. For administrative purposes, most people share a birthday of January 1st.