PART THREE–PROGRAMME FOR REFORM
Human nature is so complex that paper plans for society are to the statesmen not worth even the price of the defaced paper. Successful progress creeps from point to point, testing each step.
–Alfred North Whitehead (1861–1947)1
This book as a whole is akin to a songline and its three parts to a Dreamtime-like continuum of past, present and future. Part Three might thus be thought of as a Dreaming about the creation of a care information utility that is central to the reform and reinvention of health care for the future Information Society, anchored locally, nationally and internationally in the public domain. Reinvention requires bold imagination, linked with creative and carefully calibrated implementation and learning by doing.
This Dreaming is not yet close to a technical specification. It is a vision focused on future health care needs, a rehearsal of values and principles that such a utility should embody, and the imaginative implementation required to evolve and sustain it. The reflection in parenthesis of Chapter Five of Part One has set out context and motivation of this endeavour.
Such dreams are difficult to connect meaningfully with the concrete language of a dreamless machine and how it gets involved in health care. The openEHR and OpenEyes initiatives described in Chapter Eight and a Half were once similar dreams and are now substantially implemented and gaining traction in everyday use, spreading around the world. They and the stories of their creation might be seen as signposts and halfway houses towards the care information utility which remains to be created.
1 Adventures of Ideas (New York: Macmillan, 1933), p. 27.
8. Care Information as a Utility–What Is Needed and Why?
© 2023 David Ingram, CC BY-NC 4.0 https://doi.org/10.11647/OBP.0384.03
This chapter is in three parts. The first explores what we have learned during the anarchy of transition of health care in the Information Age and why new ideas are needed. It emphasizes the organic nature of a care information utility, distinguishing it from a technical infrastructure. Organic, that is, in the sense of ‘relating to, or derived from living organisms’ and being adaptable, evolving and humanly-centred, to serve the needs of individual citizens for supportive health care services. In this regard, it draws an analogy with the forest ecosystem of the natural organic world, which was termed a ‘Wood Wide Web’ in a 1997 issue of Nature. It makes a parallel analogy with monetary ecosystems, discussing the relevance for health care information policy of the lessons drawn by Mervyn King, when writing about the world monetary system crisis of 2007–08.
The second part of the chapter celebrates pioneers I have known and worked with, who have made notable contributions in framing and implementing new ideas for information systems, achieving iterative and incremental advances towards meeting longstanding policy goals. The third part draws together future-facing perspectives of the changing patterns of knowledge and discipline, professional practice, education, research and global village community, which will form the landscape on which the care information utility evolves. It discusses the values and principles that should guide the development of the utility, the importance of a viable means for its standardization and the difficulties faced in achieving this.
The chapter concludes with a parenthetical reflection on what matters at the heart of the interconnected and currently fragmented domains of care information services, and the dilemmas they pose. This has been characterized in other contexts of public services as the need for a unifying change of perspective, from a focus on ‘What is the matter with you?’ to one of ‘What matters to you?’
Adventure is necessary to prevent withering through repetition–learning and learned taste replacing ardour of adventure.
–Alfred North Whitehead (1861–1947)1
This is where we are today: patients exist in a world of insufficient data, insufficient time, insufficient context, and insufficient presence. Or, as I say, a world of shallow Medicine.
–Eric Topol2
The framing of government policies for Information Age health care has become somewhat witheringly repetitive, and replete with ‘learning and learned taste’! Perhaps, the lengthy chapter just past felt like that to read! I am seeking to be more adventurous, now. The above quotation from a luminary doctor and scientist with a special interest in information technology, Eric Topol, gives a vivid context for the scale and significance of the challenges to be faced.
In this, I am not comparing or criticizing any particular technologies that might be adopted to underpin implementation of future information policy for health care. Such debate is sterile; these technologies should, and inevitably will, evolve experimentally over time, albeit some more expensively and wastefully than others. I am, rather, drawing on experience and example from along my personal songline, to give personal perspective and paint a picture of the values and principles that should underpin future policy in this field. I am, thereby, principally seeking to help clarify what future endeavours should embrace and comprise, and what their purposes, communities and environments might look like. This envisioning is by no means complete.
The storyline of the book has reached a tipping point. Thus far its approach has been one of description, with focus on drawing together and connecting diverse contexts of two millennia of medicine, centuries of science and engineering and seventy-five years of the Information Age. At the end of each chapter, I have reflected, in parenthesis, on general issues and challenges faced in introducing information technology to the domain on which the chapter has focused. In Chapter Two, this was about traction in getting to grips with the application of knowledge–connecting ‘what is true with what to do’, as it is sometimes expressed. In Chapter Three, the theme was about manifold and balance, in getting to grips with new measurements and methods, as tools of science and society in the Information Age, and their impact on the balance of health care. In Chapter Four, there was reflection on purpose, as central to why and how we build and apply abstract models of the appearances of reality. In the parenthesis of Chapter Five, there was consideration of the engineer’s inventive spirit of making and doing, and how this relates to the challenges faced in reforming and reinventing health care, through the present-day anarchy of the Information Age and leading into the future Information Society. At the start of Part Two, in Chapter Six, there was reflection on how transition in knowledge about the nature and science of life and information has paralleled changing ideas about health care services, and information policy supporting them. In the parenthesis of Chapter Seven, the theme was goldrush, reflecting on serial endeavours to commercialize health care information systems during the Information Age.
In this and the next chapter, the approach switches from one of description to what might be termed a prescription–a forward-looking perspective of the nature, design, implementation and operation of a future care information utility, adaptable to the emerging and evolving needs of tomorrow. It is a Dreaming3 about something yet to be created–difficult to conceptualize since the specific purposes and goals of such a utility remain to be discovered in detail, based on experience gained during iterative exploration and incremental implementation. Its creation will thus require an agility of approach, and implementation in manageable incremental stages. The chapter ventures off-piste, to sample experience in other fields that have encountered similar challenges in the Information Age, to look for their common ground with the changing face of health care. A bit like the dog one sees racing around and exploring, connected with and on a walk with its owner, attached by a spring-loaded expanding and contracting lead!
It is easy to spend much time talking and reading about seemingly intractable problems, hunting illusory perfection of potential solutions. There must also be traction in the way such problems are tackled at scale, otherwise the law of unintended consequences may bite hard. Traction may require a mixture and balance of methods of implementation. And each method will have its own characteristic qualities–helpfully expressive of the problem domain, in some respects, and unhelpfully limiting of the applicability of what can be achieved with it, in others. Horses for courses, as it were. A good engineer guides and melds these choices, combining an artist’s aesthetic eye, a mathematician’s grip on shape and form, a practitioner’s experience of useful things and a scientist’s knowledge of materials and methods under consideration.
Chapter Seven traced a changing pattern of health care services, alongside information systems, in their transition into the Information Age–albeit a pattern still primarily determined by and focused on health care providers and their supporting suppliers of products and services. With a touch of hyperbole, the parenthetical reflection characterized this as goldrush–panning for glinting advance in science, technology, profession and industry! This has treated the data subject as a resource for serving those ends, rather more than as a person to be supported in relation to their wishes and needs for intervention and support. A new balance is needed that supports and enables people to cope better in what matters to them, as active and responsible citizens, and partners in their own health care. This chapter charts this ambition–one of an information utility centred on the needs of individual citizens, and the professional and public services they directly engage with. It explores the perspective of what this utility should look like, and why. It profiles some key pioneers encountered along my songline and their pioneering endeavours to build better information systems.
Past problems have resulted from a combination of failed traction, exacerbated by rapidly obsolescent technology, proprietary enclosure of both data and method, and failure to learn. Chapter Nine will make a case for the pooling of knowledge and a better balance of local initiative and community-led governance with national policy that concentrates on enabling and supporting methods and services which can and need to be shared, nationally and internationally. The foremost of these requirements is for a platform for capturing coherent, mutually consistent and sustainable care records, specified independently of technology or supplier of technology. It seeks thereby to chart a realistic and affordable path away from the burdensome accumulated legacy of non-coherent, unmaintainable, unduly expensive and progressively unsustainable information systems and their supporting infrastructures and services.
As tracked in Chapter Seven, the digital care record has been serially reidentified as the principal challenge of the field, since the 1970s–the sine qua non of progress. The reasons why it has serially disappointed are manyfold. The challenge, as so often in the quest for computerization, is not essentially technological. It goes to the heart of how to express, enable and support, in a computable form, what medicine and health care are, and what they do. It is then a challenge of how this reality is managed and governed. The problems thus ramify throughout the personal, professional, scientific, social, managerial and industrial domains of health care. They probably could only have been gripped successfully, centrally, at the professional level, and this has never happened or, indeed, been seriously attempted. The 1990s UK General Medical Council perspective of Tomorrow’s Doctors, that I introduced in Chapter Seven, which was considered a landmark of policy of the time, scarcely touched this issue.4 Almost by default, it has fallen to be picked up and picked over by a mix of industry, academia, national government and international bodies; very often by people who are working at a distance from the everyday realities of health care services, science and technology.
The professions of health care must recognize a greater sense and measure of responsibility to chart and lead implementation in, and learning from, this central field of endeavour, and failure, hitherto, to do so, effectively. And policy makers, more widely, must likewise recognize the failure to understand and manage the unruly and ruinously expensive, burdensome and wasteful aspects of the scene that has unfolded. Rather than a cutting to the chase, it became something of a wild golden-goose chase leading and following into Topol’s Shallow Medicine.
Here is a slide I used at a Medical Research Council (MRC) conference some fifteen years ago, seeking to flesh out strategy for tackling the challenge of implementation of digital care records:
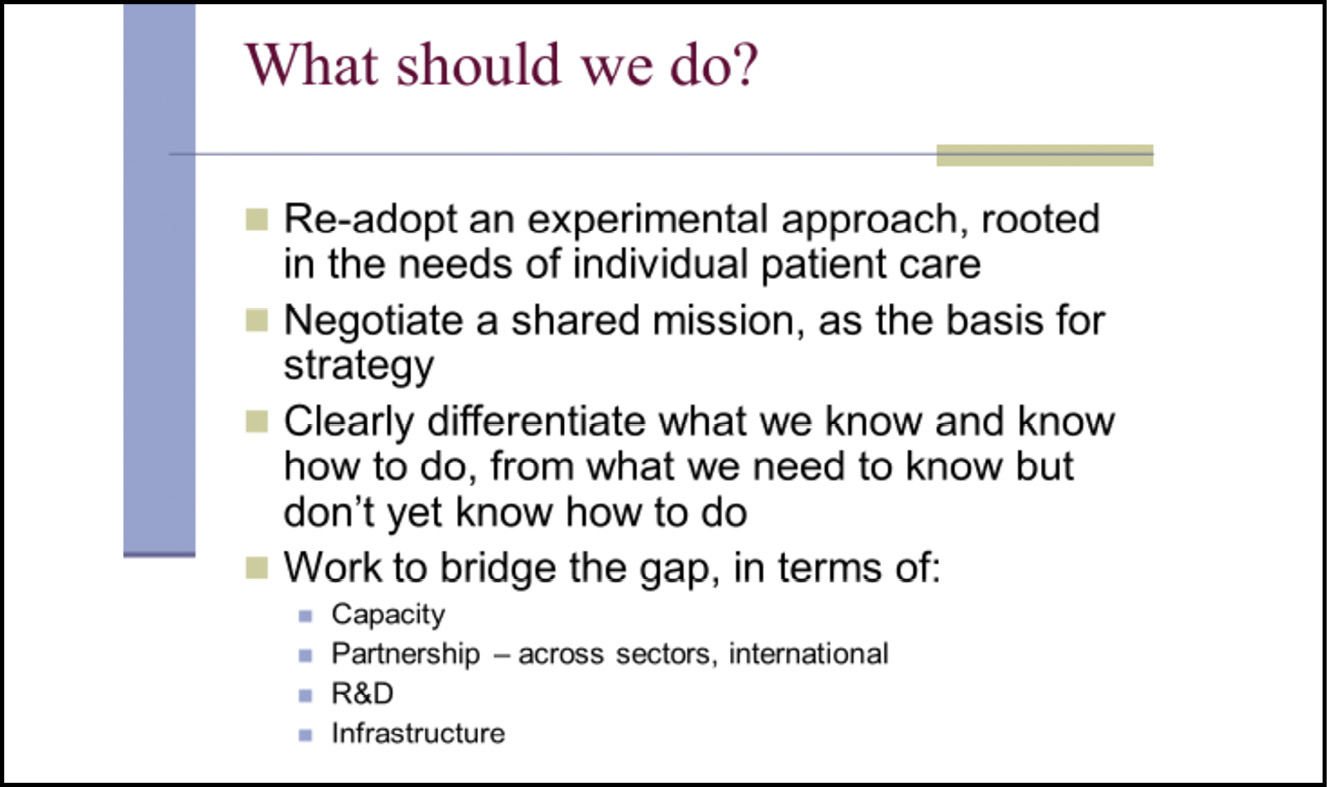
Fig. 8.1 A slide from a Medical Research Council conference presentation on health informatics. Image created by David Ingram (2010), CC BY-NC.
I also used Maurits Escher’s (1898–1972) lithograph, Ascending and Descending (1960), which, on this occasion, I interpreted as depicting zero sum, disjoint endeavours.5 Problems arise when central and locally driven policies and approaches, top down and bottom up, run contrary to one another, and become out of kilter and out of step. The ascenders and descenders in the optical illusion keep passing one another by and go round in circles! I described optimistic and now widely implemented, but then still highly experimental and exploratory, ideas for creating and pioneering a new way forward–that of openEHR. These are delineated in Chapter Eight and a Half. The ideas have evolved, improved and gained traction over thirty years, and now demonstrate global community and uptake. They have combined iterative and incremental clinical engagement and grounding in both mission and method, technical rigour in specification of implementations, and a culture of open sharing and demonstrated sustainability and affordability. They have not been created top down, they have evolved from and on newly created common ground, predominantly as an expression of wide-ranging health care related community motivation, effort and commitment. They are parables of what money and power cannot create or buy, and yet society needs and will depend on for its future health care.
Such initiatives show how it is possible, now, to restore ownership and stewardship of care records to where they belong, close to the people and communities they describe and to which they belong. They aim to position the uses of the data, such that it can accumulate value for all people and in all services, and rather does not isolate and fragment them. These initiatives have created a template example for future creativity in building a coherent and connected open ecosystem of care information as a utility–applications and data built on a technology and vendor neutral platform, that can be freely adopted, implemented, evolved and sustained, over time. This is particularly crucial in the health care domain, a quintessential example of a field for which lifelong coherence of personal data matters, as its lack can cause great harm as well as avoidable cost.
For health care, the ecosystem of information appliances and information utility that Joel Birnbaum envisaged, as discussed in Chapter Seven, might be described in simplest terms as an enabler of the best achievable and affordable health care services, for all concerned. In this, it must connect methods, devices and systems that function efficiently and effectively together, with outcomes that are useful and affordable, for individuals and for society, and with participation, oversight and regulation that is fair and appropriate. The success of this information utility will depend on the values and principles that it embodies and the manner in which it approaches its implementation and governance.
The present-day landscape of health care information systems comprises a legacy of disjoint and bespoke systems, closely integrated with complex and still current workflows of health care services that are becoming increasingly cumbersome and unsustainable. This is costly, wasteful and inefficient, and it clutters and distorts the scene. It is a pattern that has accumulated widely across society, well beyond the health care domain. We can achieve systems supporting health care services that are, by far, more effective, affordable and adaptable than have been achieved, to date. There are now technologies and tools available to be deployed to this end, that are considerably more powerful, flexible and accessible than was imaginable at the start of my songline. This chapter focuses on what this future utility should look like. The half chapter gives examples to illustrate progress in how it can be created–iteratively, incrementally and sustainably.
It remains an open question as to whether society can and will succeed in such an adventurous mission–to create a coherent and citizen-centred information utility that supports current and new services and ways of working, where technology now enables us to make and do better, while not damaging what was well made and done before. It is an open question because information technology has both transformed society and exposed and exacerbated its weaknesses and vulnerabilities. It has been explored and exploited, and society has adjusted to life like that. Zobaczymy [we will see]!6
But along with the political scientist, Robert Putnam, and knowing well the oncoming generation of our own nine grandchildren, I am decidedly optimistic on this score. In his book, Upswing, published in 2020, Putnam characterized the past sixty years in the United States as social downswing, which he described as a movement from ‘we to I’.7 This era coincided with the arrival of the Information Age. In those decades, information technology transformed institutions and their working methods and exposed them to destabilizing and destructive forces. What was promised by IT-toting canvassers at the front door, to enable better ways of connecting, working and integrating, has, when let in through the back door, created a new mess and destabilized the household. And some canny operators called at the front door to divert our attention, while their accomplices crept in at the back door to rob us!
For many, life has indeed evolved for the better, but many have encountered new burdens, fragmentation and isolation in their lives. Putnam’s extensive research and collation of national and international trends and data charts that sixty years of upswing (‘I to we’) from the turn of the twentieth century, which was followed by sixty years of downswing. Countries do not move in phase with one another, but one might reflect that, in his perspective, we may be at another social tipping point, where transition from today could, as he believes it will in the USA, coincide with a new era of upswing. In this era, a care information utility can be a powerful tool and motivator of a future healthy and caring society, helping to put right the health inequalities that have become entrenched and exacerbated–in the United Kingdom, as characterized, from William Beveridge (1879–1963) to Michael Marmot, in the past sixty years of Information Age downswing.
We need, now, to think ahead, and differently, about the environment in which the envisaged information utility will grow and operate. First, we must differentiate infrastructure from utility. The quality of the utility will depend on the quality of the environment of which it is a part. This includes, but is much more than, its infrastructure. The meanings and values ascribed to the information utility for health care are human and social in nature. The present-day divided and overburdened environment of health and social care has not been a good or easy environment in which to engage in radical information engineering.
In this and the following chapter, I imagine in more detail what an information utility and environment in which patients and professionals are partners, co-creators, owners and sharers of knowledge and capability, that can gain traction in creating a pathway into practice, would look like. We are, perhaps, halfway towards making this a reality, as I conclude in Chapter Ten.
In my Dreaming, I think first of care information utility as a forest ecosystem. Forest ecosystems illustrate many aspects of mutual creation, sharing and enhancement of common resources. Both are integral with life and living and evolve organically. In our times, the realization of a new forest ecosystem and utility has depended heavily on the motivation and mobilization of volunteers. Like forests, information utilities have communities–those that create, nurture and sustain them, and those that search, discover and consume them. They have an architecture of structure, function and connection.8
In my second dream, I think of information as a currency, exploring the human ecosystem of money. Here I discuss Mervyn King’s analysis of the reasons for the near collapse of the world monetary system in 2008, and his urging of the need for new ideas to guide its recovery. My purpose here is to see what light this history may throw on the ecosystem of information, and the need for new ideas, there.
These two dreams are quite lengthy detours in the storyline of the book, drawn together in the succeeding sections, which provide fresh perspective on the recurring problems and failures in the health care information ecosystem. Here, and in Appendix III,9 I describe how fragmented policy of the past fifty years has been framed and implemented by government, how this has played out in practice and the impediments faced. I draw on examples of great pioneers of the field and what they achieved, the environments in which they worked and how they approached their work.
The chapter then looks ahead to the factors now shaping requirements for a health care information utility, focused on the needs of citizens in their global village lives and in the rapidly evolving landscape of knowledge and discipline, professional practice and education, more widely. I highlight Richard and Daniel Susskind’s advocacy of shared practical expertise as the common ground of professional-client relationship in the future, ‘where our collective knowledge and experience, insofar as is feasible, is nurtured and shared without commercial gain’.10 I also connect with Ivan Illich’s (1926–2002) 1970s, pre-World Wide Web, vision of a web of shared resources for education in a ‘deschooled’ society. The chapter closes by suggesting the pattern of culture, principles and approach that will be needed to underpin the creation of this utility, and the common ground on which its ecosystem can grow and be sustained–open and common ground, on which its success will depend. The challenges of standards and standardization of this common ground are discussed, and the chapter concludes with a reflection on how information utility connects with changing balance in health care and society today, from ‘What is the matter with?’ to ‘What matters to?’ its citizens.
Infrastructure and Utility
The term infrastructure embraces a wide range of facilities that support everyday life. We call the services they deliver ‘utilities’, as they are widely used and useful. We hear the term used in many contexts: local roads, national railways, national electricity grids and gas pipelines and satellite communications networks. With the pervasive spread and flow of information systems and services, linked through the Internet, information itself has become a utility. Such utilities extend into every home and engage us all in the way we live our lives. As such, they are much more than the physical infrastructures through which they reach us and affect our lives.
It is important to differentiate the utility from its associated infrastructure. The distinction parallels that of structure and function of systems, more generally. Computer programs have often mixed the two in a disorderly manner–such overlaps bedevil their clarity, coherence and sustainability.
Utilitarianism is a school of philosophy that focuses attention on usefulness, in terms of the achievement of as much good as possible for as many people as possible. The movement was pioneered by Jeremy Bentham (1748–1832). In reaching decisions among multiple options, policies must come to terms with differences people have: about what is good to achieve, who creates and who benefits. Statistical methods in decision theory use the term utility as a measure of achieved outcomes, combining the value each possible outcome would deliver and the probability that it will occur in practice.
In simplistic terms, utility might be thought of as about meaning–what it means to have shelter, security, clean water, reliable communication systems and good health care services. And infrastructure is, likewise, about method–how we create and operate the utility. The principles that determine the goals and framing of a utility underpin the requirements for and operation of its associated infrastructure. These principles cannot be described in the language of infrastructure. Specification of infrastructure is subsidiary to the purposes it serves and the requirements it must meet. Information utility and infrastructure for health care function and connect within contexts of discipline, profession, community and governance. They must mesh smoothly as they are connected at the hip (in the Health Information Platform, that is!).
It is in the language of health care purposes, values, meanings and choices that we must express the requirements that the infrastructure is designed to meet. There has been a plethora of competing orchestrations of these requirements and their associated roles, responsibilities and accountabilities. As a result, the design and performance of the information infrastructure has embodied a motley, and ever-changing, collection of skills, instruments and tunes–a centre-stage, out-of-tune and often wrongly blamed orchestra, lacking conductor and lacking score. It has not scored well!

Fig. 8.2 The scope of health care information systems–domains served, regulatory perspectives and expectations of the quality of data encompassed. Image created by David Ingram (2010), CC BY-NC.
The left of this slide (Figure 8.2) depicts the scope envisaged for IT infrastructure seeking ‘connection for health’ in health care. The different perspectives in play are depicted on the right. And the expectations of their combined orchestration are featured along the arrow. Nowhere was there evidence of a coherent, rigorous, engaged, resilient and dependable plan and design for data and information flow–encompassing how, when, where and why it is used and governed, and by whom.
Infrastructure is difficult to create and manage. It is historical and circumstantial, not all about gleaming new and fast railways. I used to use this amusing story to illustrate its legacy (see Figure 8.3).
Fig. 8.3 A military analogy for the challenges faced in harmonizing and integrating disparate infrastructures. Image created by David Ingram (2002), CC BY-NC.
The challenge of creating coherent information infrastructure for health care systems is all there! This kind of challenge has faced us all in our everyday battle to keep our domestic IT functioning and up to date. We throw a lot away and bear our losses, but this is not an affordable or manageable option for health care services, in what we buy and implement there, lacking coherent requirement, scope and definition.
Whole industries engage in providing and maintaining infrastructures. Some are owned and operated in the private sector, subject to legal regulation where quality and availability are matters of legitimate public concern. Some are owned and operated in the public sector and others involve partnership between the two. There are choices and consequences implicit in each model chosen, depending on social, technical and economic context, political culture and need.
As Birnbaum remarked in his lecture at the Royal Society, when discussing the concept of information utility, infrastructure is most successful when least noticeable. The nervous system is in a way an information infrastructure and it, too, pulses away largely unnoticed, unless alerting us by design (that frying pan is hot!) or in malfunction (a sectioned nerve has paralyzed an arm). Physical infrastructure declines, visibly, with age and use. Poorly or inadequately functioning infrastructure becomes obsolete and burdensome, and this is widely noticeable by its users. Disjoint implementations impose scalar sum burdens on services and vector sum benefits for health care. Two scalars of equal size, sum to one scalar of twice the size. Two vectors of equal size, lined up and facing in opposite directions, sum to zero.
Birnbaum argued for the benefits to users of switching to a focus on information utility and information appliance, as I used to summarize with this slide:
Fig. 8.4 Advocacy for information as a utility–adapted from Royal Society lecture, Joel Birnbaum, 1999. Image created by David Ingram (2010), CC BY-NC.
Pervasive information utilities have enabled considerable social and economic gains: in education and research, delivery of products and services, access to knowledge, opportunity for personal enrichment and group participation, collaboration and cooperation. On the flip side, they have become easy targets of manipulation and corruption, channelled through rampant social media, with their owners and operators pervasively powerful and their brands profiteering. New challenge to equity has been described as a ‘digital divide’, separating those able or unable to use and benefit from information technology. It is a paradox of our times, that being more connected, digitally, has become associated with becoming more divided, socially.
As reflected in the anarchy that has reigned, and the inequalities and inequities that persist, the Information Age is shaking the foundations of the ways we live, as Whitehead said major transitions always do. There is a blizzard of alternative choices, meanings and ideas of goodness, and even ‘alternative facts’ have made an appearance. Bertrand Russell (1872–1970) believed the basis of knowledge to be truth and believed in facts. As a mathematician and logician, he had a precise reasoning mind when discussing these matters. In health care, personal meanings and contexts matter and influence strongly. And as ever, ‘what is true’ and ‘what to do’ are inextricable, but not so much Russell’s area of expertise. As recorded along the timeline of Chapter Seven, the context and balance of personally and professionally managed care has shifted in the Information Age, with burden of disease more chronic. Once quickly terminal or intractable diseases are now more manageable and survival times longer.
Observing the credulous ‘e-counselling’ interactions of colleagues at the Massachusetts Institute of Technology (MIT) who were using his ELIZA program, Joseph Weizenbaum (1923–2008) became fearful of human gullibility and error in relation to machine intelligence and personal communication. There was, he said, a hidden context that deceived and misled them. He wrote as follows:
Claude Shannon showed that even in abstract information theory, the ‘information content’ of a message is not a function of the message alone but depends crucially on the state of knowledge, on the expectations, of the receiver. The message ‘am arriving on 7:00 o’clock plane, love, Bill’ has a different information content for Bill’s wife, who knew he was coming home, but not on precisely what aeroplane, than for a girl who wasn’t expecting Bill at all and who is surprised by his declaration of love.11
Just as human communication depends on understanding human context, computer representation and reasoning with knowledge depends on appropriate and relevant machine capture of human context and meaning. This is of considerable impact in the socially connected, biologically and clinically diverse knowledge and actions of health care. For those in need of support, the boundaries between different fragmented agencies can easily become automated barricades and bureaucratic filters, disabling rather than enabling and supporting lives.
The management of publicly provided infrastructure and utility requires cooperation across many levels of organization and governance. Government spending involves choices: about method, distribution and money. In turn, it involves choices about the capability and capacity of those who provide and receive services. Constrained within finite time and resource, information for health care exhibits considerable complexity. Taming that complexity is technically and organizationally essential, while remaining clinically and socially unpredictable and potentially harmful. This intrinsic uncertainty is a principal reason why information utility and infrastructure for health care have proved so difficult to scope, design, build, operate and sustain.
And in this anarchic situation, politics, both local and national, as the art of the possible, is stretched to its limits. Those at the top of the political ladder sometimes express themselves as feeling powerless to lead and influence how policy aspirations and goals are implemented and play out in real life. It seems appropriate, here, to think more widely about the information ecosystem. First emphasizing its organic nature, through analogy with the forest ecosystem, and then as an impersonal data stream, through analogy with the monetary system. I build from these parallel Dreamings, to prescribe core elements of a future information utility and infrastructure centred on care records. The analogies are not perfect–none such are–but their comparisons throw light on the ecosystem of information utility. When one looks at the fractal structures of data persisted in care records, and their intrinsic variability from case to case, as they grow over time, and from time to time, one sees a mirror of the basic and repeating patterns of plant growth. It is a difficult challenge to build faithful and tractably useful computer software representations of this dynamic form and complexity. I am in no way suggesting that such software is itself some kind of mystical organic entity. I am using the analogy to emphasize that the information it processes is mirroring whole living beings. We must choose carefully how we seek to implement this reality in a machine.
Information Utility as Organism–A Connected Forest Ecosystem
The forest is not a collection of entities […] it is a place entirely made from strands of relationship.12
The connection of information utility with forest ecosystems lodged in my mind over the past decade, as the largest new forest in the UK was being planted, just five kilometres from our house. Heartwood Forest, as it is called, is an initiative of the national Woodland Trust charity and tens of thousands of volunteers of all ages have planted hundreds of thousands of saplings, which have now grown up to five metres tall. The volunteers were inspired to contribute to a global need for replanting of forest resource, which has been disappearing at the rate of a country the size of Denmark, every year.
Today, as I am tidying the book’s first full draft (7 May 2021), I have discovered Suzanne Simard and her ground-breaking work on the ecology of the forest. Her passion for forestry was nurtured from childhood as the daughter of foresters in British Columbia, then focused in her 1997 PhD, debunked for years by the learned in concert with their interested industry parties; she doggedly pursued this work throughout her career, and is now Professor in the Faculty of Forestry at the University of British Columbia and a recognized world authority. Her findings about the declining health of trees and their implications for forestry practice are now mainstream. The practices needed to recover the damage of years of industrial forestry and global deforestation are in their infancy. Her research established the idea of the forest as an organic information ecosystem. The echoes between her story and idea, and the story of breakdown of Industrial Age health care and idea of care information utility as an organic ecosystem, felt compelling and worthwhile to explore further, here.
Imbued with a love of trees and forest environment and the ancient Aboriginal communities that inhabited and depended on them, Simard developed an instinctive understanding of the complex and integrated web of communication and mutual support that different trees and forests embody, and the biological pathways and organisms that constitute this resilient, adaptable and productive network–over time, above and below ground. The journal Nature published her original paper and featured it on the issue cover, under the moniker of ‘Wood Wide Web’.13
Heartwood Forest is located on common land and abuts an area that was once, according to St Albans folklore, the haunt of a notorious highwaywoman, who was seeking to repair her aristocrat family finances by robbing the occupants of passing horse-drawn carriages, hastening north and south, to and from London. She was known as the Wicked Lady and we used to park our car at the Wicked Lady pub that commemorates her exploits, while walking our regimented many thousands of steps a day, in the forest and through the Spring, Summer and Autumn of our Covid year. It is now halfway to becoming a forest environment, full of trees, vegetation, wildlife, walkers and their dogs, cyclists and horse riders. It includes a newly planted arboretum of all the trees native to the UK and envelops one of the oldest ancient bluebell woods in the country. It has provided afternoon exercise and relaxation to balance the morning writing of this book.
In Chapter Five, I made connections from steam engines to information engines. Here I am making connections from forest ecosystem to information utility for health care. We use metaphors of wood and trees to describe knowledge and meaning hidden in detail–branching data structures, a forest of data and not seeing the wood for the trees. We create and consult maps of the pathways through the forest. Forests, like information systems, have uses and users. They draw together the animal and insect kingdoms and the natural world of fungi, sharing moisture and nutrition across a connected network, embodying both animate and inanimate worlds. We talk of the tree of life and pulp paper from wood.
The trees grow by drawing and sharing resources–water and nutrients from roots and fungal networks below ground, and photosynthesis from sunlight in the leaf canopy overhead, channeled through top-down and bottom-up highways of sap. And likewise integrated are the insects, animals, plants and fungi that co-create the forest and live there, and the humans who are its stewards and users who visit. This is an ecosystem of forest life, with water and nutrients as its currency and the sun’s energy as its source. Health care information ecosystems are similarly organic–the information content is akin to water and nutrients, and information flow is akin to a traded currency. In this imagined information forest, we grow trees of knowledge, integrating, sharing and communicating through roots and leaves of electronic interface, energized in computers by electrons of electric current rather than the photons of the sun.
The information utility is a virtual forest, guarded and sustained by information foresters who are its co-creators, sustainers and users. Its role is to provide useful and meaningful connections of trees of knowledge and data. Information is the currency of these connections. Trees grow from and propagate through seeds. Trees of knowledge and data are members of a virtual forest grown from a multitude of seeds, as are the trees, plants and other organisms of the living forest.
In the natural world, forests have grown and evolved, from the ground up. Trees of different kinds and scales have been created, propagated and planted. They have evolved, conditioned by use, time and circumstance. A community of foresters and ecologists, inhabitants and users has emerged, nurturing the forest, and feeding from it. In the virtual forest, we encounter hierarchical trees of knowledge and data, describe their different roots, trunks, branches and leaves, and their mutual affinities and antipathies towards other inhabitants of the forest–of discipline, function, content and use.
Trees grow from seeds planted in, and drawing nutrition from, the ground. Forests develop as flourishing habitats and engines of photosynthesis and propagation, decaying over time to fallen trees, no longer functional or useful, blocking the way, and decaying back into the ground. Information systems support life cycles of usefulness of information and have life cycles of their own.
Trees and forests that survive centuries, are organic ecosystems held together by mother trees that nurture the young and provide continuity and reliance. Forests are beautiful places. They exist above ground, in ground and below ground. They coexist with the animal and insect kingdoms and their human users. Trees differ–their canopies intersect and cooperate, and roots enmesh and communicate. New trees and old, healthy and diseased, grow, live and decline. All need water and nutrients, share common information at a cellular level and participate in global respiration and energy balance. There is a dynamic balance of sustenance and use. Information systems mesh with ways of living and working, just as patterns of mathematics and information play out in life itself. In the knowledge of their evolving balances and imbalances lies understanding of health and disease, life and death, and ways of enabling, protecting and enjoying life.
In our times, a plan to create forests will acquire and prepare the ground, in collaboration with specialists and volunteers, to choose, seed and plant the trees. It will learn about forestry from foresters, forest ecology from ecologists. And needs, priorities, purposes and feasibility–energy, construction, vegetation, recreation–must be weighed. National and commercial ambition have sometimes confabulated, looked to an imagined future of beautiful forest ecosystem, and attempted to short circuit organic growth. They have brought bulldozers to clear and prepare the ground, killed presumed competing and unwanted trees, destroying the fertile and synergistic habitat of the mature forest that has evolved over millennia. Factory-farmed saplings and full-grown trees outside of their natural ground and community have been craned into place and lowered into holes bored in the prepared ground. Fertilizer spurts early growth and then a weaker kind of forest ecosystem leads to disease and decline. I have seen lines of oak trees alongside airport motorways and in city squares in the Middle East and the water they consume. Many die quickly, unsuited to either location or use. They fail to integrate through canopy, subsoil and roots, and do not become a balanced ecosystem. Expectations, timescales, materials and methods, capability, discipline and the driving sponsorship and management of the enterprise are all found wanting.
The health information utility of today has been driven, in large part, by commercial and managerial goals, arriving akin to the bulldozers and boring machines of the artificial forest. New information utility must be grown foursquare as an ecosystem integral with health care communities of practice, drawing on the connections of people, disciplines, professions and ancillary services, including the supporting industries, that come together to enable them to function as needed and desired. A sound ecosystem can be replenished and supported efficiently. An artificial ecosystem costs hugely, initially and over time, is not resilient and often does not fulfil what was hoped for from it and depended upon. I have seen pedigree herds of cattle producing the most amazing milk, feeding on alfalfa grass at an oasis deep within a life-threatening desert of Saudi Arabia, and hydroponics greenhouses producing useful salad crops, there, too. Careful engineering to match ecosystem with environment and community pays dividends. I will write below of people I have known who have achieved this in information systems.
Simard’s story, with its experimental underpinning that fills out her concept of a Wood Wide Web characterizing forest ecology, is transformative in its implication for care information utility. In the patterns of material, energy and information flow that she has lovingly revealed lies an important message for the Information Society. And in her description of the destructive impact on forest ecology of forest management of many recent decades is an analogy of the problems that the machine imperatives of the Information Age have brought in care of the individual and the communities and practices through which it is sustained. In this analogy, the trend of Globalton life might be seen, apprehensively, as a deforested Localton, stripped of its mother trees and the communication and nurturing that sustain health and resilience.14
Two further threads illuminate the way ahead towards creation of the care information utility; the first about values and choices, and the second about focus and creation of options.
Paths through the Forest
In 1915, the poet, Robert Frost (1874–1963), wrote a poem entitled ‘The Road Not Taken’. It was for his poet friend, Edward Thomas (1878–1917). They used to walk together. It starts like this:
Two roads diverged in a yellow wood,
And sorry I could not travel both
And be one traveler, long I stood
And looked down one as far as I could
To where it bent in the undergrowth […]15
As the story goes, Frost claimed subsequently that it was written in jest, to chide his indecisive companion, who often could not make up his mind about the route they should take and, after the walk, talked with regret about how the route they did not take would have been better. Talking the talk and not walking the walk, as it were! Too much talking and too little walking, or too much walking with too little talking. It is not easy to balance the two. The poem has been multiply-dissected, verse by verse, to cut out meanings perceived by its readers–as with mine, here, as an allegory of choices made when walking through life. Apparently, Frost was taken by surprise by this depth of study of his joke, but he also purportedly said ‘I’m never more serious than when joking’, so, who knows? Literary clowning is sometimes used to camouflage serious intent.
In the case of a walk through some wood, sometimes there is a single bifurcation of the route ahead and sometimes there are more options, all looking feasible to be followed, one at a time, adding to experience in successive visits over time. If we think of the forest as a wicked problem domain, and each walk as an attempt to resolve the problem, each walk changes the available paths, so it may not be possible to retrace or repeat steps. A choice is made, implicitly or explicitly–it is one way or another. Choices are often cast in the light of bifurcation, and decisions line up fifty-fifty, indicating either ‘don’t know’, or, in a style as described by Primo Levi (1919–87), one half convinced of one and the other half of the other, repelling one another to greater extremes of divergent opinion.16
These choices are not like the double-slit experiment that pervades descriptions of quantum theory, where the electrons, in some sense, follow a path through both, like a wave of water, and producing a similar interference pattern when observed on the other side. That is hard to reconcile with appearances in other experiments, of the electron as a particle. If the observer sets out to observe which slit each electron goes through, the interference pattern disappears. The electron as particle view of reality and the electron as wave view, each seem to make sense as interpretations of some experimental set ups and not others. How can theory that is so astonishingly successful in predicting outcomes observed, be so unfathomable as to what it means in terms of the nature of the underlying reality itself? As discussed in more detail in Chapter One, when introducing Robert Oppenheimer’s (1904–67) 1954 Reith Lectures, science has to live with that complementarity, about different ways of looking at and reasoning about appearances and choosing between them.17
Even poets cannot actually walk along both paths through the wood, simultaneously, to weigh them up. But from a different viewpoint and perspective, maybe from a helicopter, for example, they could experience a pattern emerging from the two, together. Maybe the two taken together in this way would prove a better option than either taken alone. As attributed to the author, F. Scott Fitzgerald (1896–1940), in ‘The Crack-Up’, published in the New Yorker Magazine (1936), ‘The test of a first-rate intelligence is the ability to hold two opposed ideas in the mind at the same time, and still retain the ability to function’.
There are choices to be made about the path we take to shape the future information utility, that cannot be avoided. Only by exploring the possibilities in a full and principled manner, can we weigh their merits. We must engage first at the level of principle, express it as simply as we can, and go from there. The following, from the concluding page of Richard and Daniel Susskind’s inukbook, which is discussed further below, is about two paths in the road ahead for professional culture in the Information Society. It is about matters of principle. I cannot say it better:
Beyond the professions, there will lie a fork in the road, with two possible routes stretching out. One leads to a society in which practical expertise is a shared online resource, freely available and maintained in a collaborative spirit. The other route leads to a society in which this knowledge and experience may be available online, but is owned and controlled by providers, so that recipients will generally pay for access to this resource and our collective practical experience is enclosed and traded, most likely by new gatekeepers.18
Thus far, we have largely been shepherded along route two. The information utility for health care is so intimately bound up with human society that route one should be given a better chance. Here are the Susskinds, again, in their final chapter, talking about living and evolving treasure troves of knowledge, empowering citizens to live healthier and happier lives–my forest ecosystem of information utility:
We feel a great sense excitement in imagining human beings across the board–rich and poor–having direct access to living, evolving treasure troves of help, guidance, learning, and insight that will empower them to live healthier and happier lives. But this shift will not come about spontaneously. It is a goal to which we must actively strive. We must remember that inaction, as well as action, is a choice […] the potential sins of omission here are too profound to ignore. We now have the means to share expertise much more widely across our world. We should also have the will.19
We use the expression ‘my way or the highway’ to express our convictions about paths ahead of us. Highway One encircles Australia. People in retirement sell their houses, buy motorcaravans and live on the road, encircling this route. Bożena and I chatted to some of these peaceful and contented folks who we met on one of our holidays there. For them, Highway One seemed a safe and enveloping circle for their lives. I do not know where Highway Two goes to in Australia, but hopefully somewhere safe!
Hedgehogs and Foxes
Around 1953, the philosopher Isaiah Berlin (1909–97) published a scholarly essay entitled The Hedgehog and the Fox, drawing on a classical poem of Archilochus (680–645 BCE), in which he says Multa novit vulpes, verum echinus unum magnum [A fox knows many things, but a hedgehog knows one big thing].20 Berlin used the hedgehog/fox classification to categorize great writers. His readers took it much more broadly, to be allegory of meaning and truth. Matthew Syed, writing in the Sunday Times, has Berlin’s hedgehogs reducing everything to one idea and filtering out everything else. His foxes, by contrast, run with lots of ideas in different contexts, seeing how the pieces fit together. He takes Berlin to imply that:
It is psychologically easier to be a hedgehog, but to understand a complex world, it pays to be a fox. And that neither meaning nor truth is contained in bare facts, assertions, datapoints, viral clips and simplistic headlines: rather, truth is contained within a context–how one thing relates to many other things, and how parts fit into more complex wholes.21
This idea echoes with David Haskell’s idea of forests as made from strands of relationship, and to Carlo Rovelli’s idea that physical reality is best expressed through relationships. Berlin, himself, commented ‘I never meant it very seriously. I meant it as a kind of enjoyable intellectual game, but it was taken seriously. Every classification throws light on something’.22 So, who knows? I tend to agree with Syed, though.
We all classify when seeking to simplify, make tractable and cast light on complex phenomena. On their walks, Frost and Thomas might have encountered hedgehogs and foxes. I am not suggesting hedgehogs populate one route and foxes another, by the way! Maybe Frost and Thomas are fox and hedgehog, or hedgehog and fox, for that matter. In life, the hedgehog does move slowly and rolls into a bristly protective ball, and the fox does move faster and range wider, some silver and some sly. We have both hedgehogs and foxes in our garden–the hedgehogs live there and sleep at this time of year. The foxes make a lot of noise and visit, sometimes attacking hedgehogs that venture out in winter, as happened last month, sadly.
Where have we got to, though, with these poets and philosophers engaging through jokes? At one rather serious evening gathering, I tried joking about the perceived dualisms and dichotomies of health informatics standards: digitized messages passing between information systems; information models that define those systems; controlled terminologies to capture the content of records. As Berlin said of his fox and hedgehog classification, these informatics classifications do throw light on something, but they are not meaningfully battled as dualisms or dichotomies. They are mixed realities, in need of investigation by hedgehogs and piecing together in context, by foxes.
Health informatics discipline has, perhaps, taken itself a bit too seriously and assumed precision of language and classification beyond what is real in the world of health care. It has become skewered on matters of ontology in description of health and disease, and ‘polychotomy’ in classifications and kinds of classification of these. Such may throw useful light on, and help organize, the appearance of the scene but are often of less help in navigating the real world of health care needs. More data, of however high quality, does not necessarily equate with better health care outcomes.
If we want to reach a tractable consensus between foxes and hedgehogs, we have two choices. Just allow time to pass, hoping to know them better by their fruits, and live with them for now, warts and all. Or seek better understanding of their differences, now, and find common ground between them, on which to chart the path to be followed ahead. Making time the arbiter is not a good idea with wicked problems. These mutate, and evidence elicited to guide choices becomes either irrelevant or remains disputed in its usefulness. We have sometimes made bad choices and reacted like hedgehogs, burrowing into the undergrowth, and digging deeper. Some wily foxes have claimed to be, and camouflaged themselves as, hedgehogs, and vice-versa, which has not helped, either. It has all been very expensive and very burdensome.
A colleague and friend, illustrious in health informatics, who has had a serious illness to contend with in his retirement, commented to me in a recent letter about his observation on the ward, while a patient, of the struggles the clinical teams had with the IT systems in use there. He expressed his sense of disappointment, shared, he said, by other colleagues, that this situation should have pervaded so far and persisted so long, as an outcome of so much effort over his career to build IT systems that would assist in the management of care. He has been mostly hedgehog in his career, and I have been mostly fox. The combination of both, and the common ground they create, is crucial for information utility to become a practical reality.
Information Pandemic–Parallels with Recurring Crises of the World Monetary System
In his book, The End of Alchemy, Mervyn King travelled along the timeline of his career as an economist and banker, latterly as Governor of the Bank of England.23 He reflected on the origins of recurrent financial crises in world economies. These he described as ‘a long series of financial crises since our present system of commerce became the cornerstone of modern capitalism’.24 They culminated most dramatically in the near collapse of the world’s banking system in 2008. He diagnosed this failure as primarily a ‘crisis of ideas’, rather than as a technical crisis or policymaking failure and mistake.
His book describes the foundations on which the monetary systems of the world now rest, following the crises of twentieth-century World Wars. It is an eyewitness participant’s account of how these foundations were shaking, with the banking edifices constructed on them and the actions of those shoring them up, no longer fit for purpose. The tools available and being deployed were, he believed, an alchemy born of a mixture of hubris and pretence of knowledge. He quoted Edward Gibbon on the invention of money in classical times and would surely have appreciated Robin Lane Fox’s recent book, also today at my side, in relation to the invention of medicine and the elixir of life in ancient and classical times.25
These stories of medicine and money form an interesting conjunction of narratives–about their origins and evolution, and how they are playing out in the Information Age. In our present-day context, they juxtapose the Marmot Reviews’ critique of failures of the health system with King’s critique of monetary system failures. Today, the admixture of cryptocurrency, blockchain and quantum computation is a new alchemy, challenging and testing the foundations of value, principle and trust on which the systems of money and health care depend. And threading through both these narratives is the story of information.
King’s book came out in 2016, eighty years after Whitehead had written Adventures of Ideas. When thinking of ideas, it is good to reread the latter’s book. Here, we find that: ‘[Great ideas] start as speculative suggestions in the minds of a small, gifted group’ and ‘Great ideas enter into reality with evil associates and with disgusting alliances. But the greatness remains, nerving the race in its slow ascent’.26 Great ideas, speculation, dangerous associates and alliances all connect and resonate with money. What, then, went wrong with the idea of money that had powered society’s slow ascent, but then tipped it into ‘crisis of ideas’ and fast descent? What were the evil associates that overwhelmed the great idea?
Money arose from local trade and barter. It had trusted form, ownership and value in this context. It provided a currency, both to facilitate flow and lubricate trade, and to be distinctive, beyond counterfeit. It opened the way to standardization of prices–everything had a price. It opened the way to markets and exchanges, for commodities, products and services and for money itself. Buyers and sellers shook hands and money, goods and services changed hands, and that is what mattered to their owners and users. Trade and money markets spread, within and between countries, transacted in multiple currencies.
Gold as currency had trusted value and was a natural, cautious choice to underpin money when trust in different currencies and their tokens of value came under threat. Money, as King says, is ‘stuff’. But stuff happens and in waxing and waning times and situations, the exchange value of money floats up and down, too. Money itself was traded. It was lent and borrowed, at a price, by money brokers. Rather than keeping money under the bed, it was entrusted to banks, banks became brokers in the economy of money, and the economy of trade and the economy of money linked and floated in sometimes tight and sometimes loose equilibrium. Governments anchored these markets and central banks stabilized these equilibria, within and between currencies and underpinned by a bedrock of gold held in vaults.
The citizen carried coin and paper–the paper itself carried a written guarantee of its value in the currency. An ever more intricate ecosystem evolved. In city financial districts, it was transacted on foot between offices and buildings with paper as the trail. Elsewhere, the central bankers lugged gold bullion between stacks labelled for their different owners and held in fortress vaults, to balance the accounts. Profit secured on foot depended on how fast you could run and whether your door knock was answered at your destination. Were you trusted in the transaction?
The computer arrived as a new money broker’s runner, with lots of new ‘stuff’ up its sleeve, poised and positioned to happen in the markets. Over time, profit by computer transaction came to depend on microsecond differences in how fast you could execute trades. Insider trading came to mean inside track in speed of access to the central database recording transactions. I knew some people who designed and coded these systems. They were seeing opportunity and doing a job, but it was coding for an accelerating flux of unknowable futures emerging from Pandora’s box.
A global ecosystem of trading has evolved, dealing in money and commodities, debts and surpluses, profits and losses. This system is enacted by quick-witted, unseen, possibly heard shouting traders, who may not always be considered the most trusted or trustworthy actors. This new style of brokerage brought a new scale of breakage. Local bubbles, even those on a South Sea scale, can burst and have global ramifications, much like the rapid spread of Covid-19 infection. The alchemy of chemically immutable gold metamorphosed to alchemy of computationally immutable bitcoin, alongside other strange non fungible tokens of value (NFT).
Money was the utility; the banking system was the infrastructure. It ruled over a complex balance and equilibrium, increasingly fragile, easily disturbed and perturbed. The prices for exchange of food and other commodities went up and down, daily, according to the weather and season. Brokers of insurance mitigated and traded the risks that the traders of money and commodities incurred with these fluctuations. Traders in the exchange of goods and services became ever more adept at buying things cheaply and selling them at a profit, and then in making artificial purchases and sales, for immediate and future closure of contracts at a net profit. They gambled to buy now, with the expectation of selling later at a profit, as traders always had. They entered into contracts to sell things they did not possess, or had borrowed from someone else, at a price, with a promise to deliver them at some future date. In this set of transactions, they had the expectation that when the time came to make the promised delivery, and thereby close the contract, they would be able to buy what they had already promised to sell, but at a lower price than that at which they had already agreed to sell it, thus securing a net profit.
Bulls and bears of trading markets became adept at exploiting loose equilibria, to push, pull and nudge prices up and down, to their advantage rather than that of the commodity producer and consumer. Multiple markets enmeshed: markets trading shares in company ownership, markets trading the commodities, products and services in which those companies themselves traded, markets trading risk and markets trading money. The alchemy of money transacted on paper and in database records underpinned these brokerages and breakages. The central banks were lenders of last resort, but their gold of last resort was sold, and its role evaporated away, increasingly leaving debt recorded in ledgers and then in databases as the foundation of their trade. King suggested that ‘pawnbroker of last resort’ might provide a better description of the central banker’s role!
Trust became subjugated to global power, brand, and clout, a trade guild tending towards a gilded money mafia. Agile, hard-working, hard-pressed and predominantly honest wits propped up the edifice, as its foundations in trade, trust and equity were washed away beneath. Equilibrium likewise disappeared and was propped up with ever more desperate artifice. It is a large system and has inertia. It is like an oil tanker that cannot be shifted quickly in its course, but it also encounters rocks of stuff that happen and quickly sink it, polluting the economy with the spilling of money. Oil and money, too, have been closely linked! And as I write, now, armies of social media-coordinated small-scale traders tweak the tail of reptilian hedge fund operators, to squeeze their massive, short trades. An army of Davids, slinging billions of ping-pong balls to cause pain and discomfort to well-healed Goliaths, both calling Foul! and Unfair!
King explains the nature of financial alchemy as a product of disequilibrium, radical uncertainty (that maybe translates as anarchy) and the Prisoner’s Dilemma of trust. He proposes policy to raise productivity, rebalance economies and reform money and banking–he calls this ‘audacious pessimism’ and says that if not adopted, rational pessimism will prevail. Weighty reviewers have applauded. Lawrence Summers, who held similar high office in the USA, said ‘Mervyn King may well have written the most important book to come out of the financial crisis’. King argues that: ‘[although money and banks] have provided the wherewithal to accumulate capital–vital to economic growth–they have done so through financial alchemy, by turning illiquid real assets into liquid financial assets’. And that ‘because they are man-made institutions, they can be reshaped and redesigned to support a successful and more stable form of capitalism’27
I am not persuaded by Marxist critique, either, as it does not seem to balance well with crucibles of enterprise and new ideas. But he had a point about the exploitative potential of capital and capitalism. Ownership of money has disproportionately further enriched the richest, spread and sustained more widely and thinly through the middle classes, and impoverished and further disadvantaged the poorest. The landscape of health inequalities mapped in the Marmot Reviews is strikingly parallel. These parallel trends have come together in crisis of the Information Age.
In one respect–probably the most important one–there is a complete parallel. Brokerage in all domains, at all levels, depends, one way or another, on trust. And breakage of brokerage is breakage of the trust that underpins it. Stuff falls apart and the central bank cannot hold. And William Butler Yeats’s (1865–1939) gloomy foreboding is that then ‘mere anarchy is loosed upon the world’.28 It is as simple (and complicated) as that! That is where ‘rational pessimism’ sets in. That is why reform must be ‘audacious’.
What would be a good metaphor of crisis of information for the modern mariner, I wonder? Maybe something like T. S. Eliot’s words, as quoted on the front page of King’s book:
The endless cycle of idea and action,
Endless invention, endless experiment,
Brings knowledge of motion, but not of stillness;
Knowledge of speech, but not of silence […]
Where is the wisdom we have lost in knowledge?
Where is the knowledge we have lost in information?29
Why all this diversion and panegyric? What is the connection between money as currency, in the way it has evolved to underpin an ecosystem and equilibrium of trade and exchange, and the ecosystem of health care information–apart from both being associated with sickness of some kind? King called for new ideas about the financial system. What can we see in his story about information as currency in the Information Age? What is the alchemy of information? How is it traded and brokered? What is its role as currency of health care systems and services? How does it differ–what are the reasons for alchemy of information, and what are the policy levers to enact change?
Health care systems today are both adventure and crisis–clinical and technical adventure, organizational and socioeconomic crisis. Both adventure and crisis have accelerated in the transition into the Information Age. Care information utility is an important key for unlocking the wicked problems arising in this adventure and crisis of ideas in health care. And as with the collapsing bank infrastructure, the infrastructure of information in the health care system is ever more pressed. Health professionals are the runners on foot, and patients and citizens are awash with Weimar Republic wheelbarrow loads of devalued information currency, disgorged, not from bankomats, but from ‘informat’ machines. And everyone else is somewhere in the clouds, devising new ‘informats’, pulling policy levers that connect reliably with expense but less reliably with desired and enduring health outcomes, seeking to regiment the flow.
In ancient times there was little by way of information or knowledge on which to envisage and base an ecosystem of care information utility. Bodies as systems and diseases as disorders were not recognized, and what was seen was believed to be evidence of the actions of mystical deities. Doctors emerged as actors in folk medicine, as Lane Fox well describes,30 with his delightful whiff of classical pedantry and hauteur! His is the story of the invention of medicine, from the times from Homer (c. eighth century BCE) to Hippocrates (c. 460 BCE–375 BCE) and the classical texts of the Epidemics associated with him. These are stories about individual patients and evolving knowledge, clinical methods and record. His account pegs information in matters of health care to its earliest origins. Citizens fell ill and needed care. Their health care was not a matter of barter and trade. Healers treated conditions; it was a service and had a value. The words that went between patient and healer were an exchange and the story of how this translated into a currency of monetary exchange, in ancient and classical times, is told in scholarly detail in Lane Fox’s book. It is an interesting and closely contextualized story.
To describe information in terms of exchange and record, within a complex ecosystem of health care services, and to compare with exchange of money, is an abstract analogy, not to be pushed too far. There are many more dimensions in play. The equilibria that health care systems depend on are multifaceted, complex and subtle. In their origins, though, there was motivation of barter and exchange, albeit sometimes with deities–a good sought and a sacrifice made. Over time, doctors stepped on to the pedestal of gods and money changed hands.
Barter and exchange depend on mutual trust and understanding of value. There are many kinds of transactions and relationships in play in health care, dependent on these. They are created and sustained on both sides. The services that exist around us, our knowledge of them, and belief and trust in them, reflect our needs, abilities and desires to either handle tasks ourselves or depend on and commission others to assist us in accomplishing them. These many relationships play out in the context of family and friends and draw on both personal and impersonal services available and affordable to us. This is where information disequilibrium easily takes root. The information experienced in the personal world, and that experienced in the professional world of health care, have separated too far apart. The exchange has lost trust and meaning, and the information system, like the banking system, has become an agent for containing and propping up the disequilibrium. If there is to be greater trust, these worlds must connect better.
It is disequilibrium of the information, not of the transaction itself. At its heart, it is not an exchange of money; money as currency does not capture the value of the exchange to the patient. But of course, it does govern access to and management of services. The industrial age of medicine has created a huge money-based market and economy of health. The result is that approaching towards twenty percent of GDP can be expended in exchange for outcomes achieved that are not correlated well with their cost. The highest in cost among the world rankings of health systems, comes quite far down the rankings in terms of outcomes achieved. Professionals have become entrained as traders in this progressively unequal and unsustainable market. And the recipients of care greatly value the care and support of friends, family and volunteers, which do not appear in the economic appraisals of health systems and the policies adopted for them.
King’s book was published in 2016 and the ‘stuff’ that has happened since–notably, political mayhem, increasing climate concern, viral pandemic and war–can only have compounded his concerns. He articulated his sense of radical disequilibrium in the world economy and the need to move from an economics of ‘stuff’, born of a time of expectation and trust in achievable equity and stability, to one of ‘stuff happens’, in an era of disequilibrium and Prisoners’ Dilemma, where capacity to cope is as important as capacity to manage. He is powerful in his analysis of the dynamic processes in play, reflecting within structures of economies and markets. He sees information technology and bioscience as positive contributors to new means for rebalancing these structures, in terms of productivity. He does not seek to make any of the connections with health and wellbeing that I have made, here. To paraphrase King and echo Ivan Illich (albeit I acknowledge, that they would have been rather unlikely bedfellows!), we might describe information pandemic and recurrent failure of national programmes for health care information technology as ‘a long series of information crises since our present system of industrial medicine became the cornerstone of modern health care’. Crisis in health care is, as he diagnosed of finance, increasingly a crisis of ideas that do not gel, reflecting in current alchemy of practice. They are exposed and exacerbated in the burden experienced by professionals and the persisting social inequalities of health catalogued in the Marmot Reviews. Both need deeper overhaul and reform than that of policy and technology.
To what extent is the crisis of ideas that King diagnoses as the alchemy of money one and the same as that in a parallel alchemy of information in health care? Is it crisis at a deeper level, enveloping both money and information, manifested and let rip in our societies from the Pandora’s box of transition into the Information Age? Polemic, again, just to emphasize the urgency of the question, but worth pondering!
King cites four areas in which, he suggests, we require audacity of pessimism, to combat the rational pessimism which he sees as underlying the imbalances at present. He sees rational pessimism reflected in how citizens respond to the economic forces they battle in their daily lives. His focus is on productivity, trade, national flexibility, and is optimistic that a sustainable equilibrium of money and economy can be achieved because of the new potential of technology to improve life for everyone. His four areas are his prescription for restoring value and ecosystem of economy and money. He discusses the paradox of policy, in which, too often, policy focused on short-term gain does long-term harm. Simard’s demolition of forestry policy showed how it resulted in short term profit from timber and long-term decline of timber quality and forest health. King sees much policy as focused on false belief about the nature of the system as a whole. He has clear ideas for the top-down priorities for stabilizing money in the short term but sees these only achieving their ends if there is radical change in life, as seen and experienced from below.
Policy currently aspires, but struggles, to be SMART in its objectives–i.e., specific, measurable, achievable, realistic and time-bound. Those engaged and experienced in its exercise, swing, he says, between youthful, hubristic optimism and aged, tired fatalism. King is in favour of new thinking and strategy based on coping rather than shaping–listening and responding to narrative rather than analyzing and predicting what we do not and cannot know.
Whitehead described ideas as adventures within sociological (human and humanitarian ideals), cosmological (encompassing laws of nature) and philosophical contexts. His concept of civilization is as a reflection of ideas, expressed in terms of truth, beauty, adventure and peace. How we pursue ideas is as influential as the ideas themselves. We all have our own, different ideas and pursue them differently. He wrote that ‘The history of ideas is a history of mistakes. But through all mistakes it is also the history of the gradual purification of conduct’.31 In life, we talk of costly mistakes and the cost of mistakes in the information era of today are ever greater, because they connect faster and more widely. The mistakes of the financial crisis of 2008 were immensely costly in monetary terms, as are the direct and opportunity costs of information systems that impose burden and legacy, while not delivering comparable benefit.
Reading, once more, King’s reflections on money and Lane Fox’s account of the invention of medicine, it seems a good point to reflect on reasons why there has been serial failure of policy for health information infrastructure and utility; why these have been so difficult to frame, design, implement and sustain.
Symptoms of these failures are revealed in plans that falter, repetitively, and at different levels of process and delivery, adding a new burden of cost and legacy to already overloaded service capabilities, failing to meet targets, deadlines and budgets. They are, more tellingly, revealed in failure to learn from failure–in repetitive mismatch of aims and aspirations with investments made, teams appointed and approaches adopted. They reflect in the observations in the 2002 Wanless Report, as discussed in Chapter Seven, showing health care far adrift in its use of information technology that is now a sine qua non of so much academic and commercial work, and of everyday life.
Continuing this thread, I review what has happened to date and set out priorities for care information utility and infrastructure in the future. I consider how each might connect with life in the evolving global village. The story of serial failure of increasing national investments in information infrastructure and utility for health care in the UK, is set against the timeline of changes in National Health Service (NHS) organization, through some eight acts of Parliament, along my timeline, since 1945. I present examples of leaders I have known, in both medicine and information technology (IT), who have demonstrated and clarified the domain. I link changes to evolving international standardization. To illustrate this thread in the book, I describe examples of integrative approaches to care information platforms and methods, that are starting to emerge widely across the world. I describe the pioneering endeavours on which these approaches have built. This then leads into Chapter Nine, which addresses how, where and by whom a future care information utility can and must be created and sustained.
Recurring Troubles of Health Care Information Policy
Health care information policy is an international challenge that transcends geography, language and markets. Its troubles have reflected, and reflected in, increasing imbalance of health care services. They signify what King termed radical uncertainty. There are, today, 2020s 20-20 costs–up to twenty percent of GDP is spent on health care services and up to twenty percent of health care professional staff time is devoted to gathering, managing, using and sharing information, and, as mentioned in Chapter Seven, the Deloitte Consultancy has estimated that over twenty percent of expenditure on health care in the USA is wasted. At a Royal College of Physicians meeting in the mid-1990s, at which we both spoke, my colleague Jan van Bemmel estimated the worldwide market for health IT products and services, mainly centred in developed economies with advanced health care systems, at in the region of one hundred billion dollars per annum. This is now estimated to reach four hundred and fifty billion dollars by 2025.
It is not that the problems have lacked priority. Renowned figures in academic medicine have chaired government enquiries around the world. In 2004, President George Bush established the Office of the National Coordinator for Health Information Technology. One of his clinical advisors came to talk to me several times and sent me the very ornate White House Christmas card, which I keep, to impress the grandchildren–though I doubt they are! President Barack Obama commissioned a national effort to improve clinical records. Asked to describe the greatest health care policy disappointment of his eight years at the White House, he said it was the failure of this multi-billion-dollar programme to make progress. Some of the largest and most successful computer companies and consultancies have entered government-created markets for national health IT systems and infrastructure. They come and go, as money taps are turned on and off and the Gartner technology consultancy hype-cycles of new technologies play out.
New computer-based devices and systems to support well-defined activities–radiotherapy, medical imaging, laboratory analysis, patient monitoring and drug infusion systems, robotic surgery–have become enduring success stories. And where these successful devices need to share data, standards have evolved across competing companies, governed by industry standards boards. Successful portable information appliances are scaling to world-wide markets.
Going up a level to the computer systems that integrate clinical work within specialisms, the problems faced are of a different order. In a perhaps extreme example, but used here to illustrate the situation more generally, one might track information for a patient brought by ambulance to an Emergency Department, admitted along with information recorded by the ambulance paramedical staff, en route. While the patient is cared for there, procedures are enacted and data is captured and recorded in a departmental record system. These activities may involve data acquired from the patient and those accompanying them. It may be acquired from, or supplied to, other hospital departmental systems, and searched for from further afield. Entries are likely to be registered in hospital-wide patient administration and management information systems. And then the patient is moved to another ward for onward care, and these processes repeat there.
According to one of my long-standing and pioneering consultant colleagues in Emergency Medicine, from the time of their admission to the Emergency Department, to transfer to the next ward, a patient’s data has, typically, already passed through some thirty different IT systems. Here, and elsewhere in similar specialist hospitals, there are typically of the order of five hundred different computer systems connecting with patient care in one way or another.
Consider then, that many of these five hundred systems are technically archaic, still ticking and operated by staff knowledgeable about how to use them, but now obsolete. Out of date in meeting present day requirements, lacking in formal specification, based on hardware and software tools, programs and expertise that are no longer available should problems arise–all increasingly difficult and expensive to service and maintain, or replace when they ultimately fail.
Consider another patient visiting London from their home in St Albans, who falls and breaks an arm, is taken to an Emergency Department. Images are acquired, the fracture is set and they and their partner are accommodated overnight as a precaution, then discharged home next day, with an appointment made for follow-up care in the fracture clinic at a district general hospital nearer to their home, to ensure continuity of care. Attending for the appointment several days later, none of the record from the acute event has been transferred to the new clinical team. Consequently, lacking that information, they conduct fresh imaging as a precaution and rebook the appointment for another time. And to get the information into the patient’s general practice record, once this episode is resolved, requires further letter-writing, to patient and general practitioner (GP). All this has probably at least doubled the time, cost and inconvenience incurred within the ecosystem, for want of a connected information utility. And it has further exacerbated, commensurately, the information explosion, heating the water surrounding the cloud data centres placed on ocean floors to dissipate their heat. And the Cloud is accelerating an approaching electrical energy crisis.
These issues also affect private sector services and their interconnections with public sector services–internationally and not just locally or nationally. Due to pressure in meeting demand, there is inevitably a growing mixed economy across all public and private sectors. This reinforces the imperative to build towards a utility focused on the needs and wishes of citizens and their records, and not one centred on providers of services and their needs and interests.
Alongside imbalance and discontinuity of delivery of care has evolved parallel lack of coherence of the information held about care. These mutually reinforce and amplify one another and the burden on health care resource increases. A large amount of money is wasted through inefficiency and duplication of processes, and their knock-on consequences throughout society. At a national level, the picture is of diverse health care providers and workforces struggling to maintain services at a local level, and central services struggling to curate and operate compatible national information resources, seeking to support local services and guide central policy. And the management of all these processes is tied up within financial and legal process and regulation–a similarly ramifying administrative burden ordained to ensure efficient and accountable use of money, that also adds to costs.
There then easily ensues institutional paralysis. Efforts to improve and adapt services have been described by ministers as pulling ‘levers of jelly’, when referring to the edicts issued in managing the current Covid crisis. The Test and Trace service allocated billions to centrally contracted national logistics organizations. It did not work as expected. The quickly exemplary vaccination programme has built on local collaboration–facilities, professionals and volunteers, GP practice by GP practice, district by district, combining local and national logistics and expertise. It has progressed remarkably smoothly, and many can justly claim credit. One thing that I was told had failed, according to the cheerful GP who first vaccinated me, was the central IT records system placed there in support. This had crashed through overload, necessitating paper backup and subsequent keying in of data, and unreliable national statistics about its progress, day by day.
The changing pattern of requirements for health care services exacerbates these problems. New initiatives attract funding and promise benefit. Meetings, conferences and publications about these, very many of which are not pursued beyond prototype, further escalate burden and information explosion across the service. The complexity and scale of the challenges to information policy is easy to describe in stories like this, and hard to deny. In many respects, they are impossible to rationalize and resolve, other than in an evolving, locally-centred environment and context. This is where the information utility of the future must be created and grown.
A key goal of the examples I set out in Chapter Eight and a Half is that they should exhibit public domain methods and solutions which are of international application and relevance, to engage worldwide communities and assist national developments. They are doing this by creating an international currency of care information, thus enabling local initiatives to build compatible, home-grown systems, or mix and match from commercial markets for products that do not tie their data to technology choice or commercial supplier.
The aim is to seed a new balance of public and private cooperation and collaboration–a diminution of proprietary enclosures of data and an opening of new common ground. There will, I believe, be much greater rigour, engagement and trust in an open ecosystem, and much greater benefit, value and safety in its adoption. I have characterized this as a 10:10:10 ambition–ten times the benefit at a tenth of the cost, and ten times more agility in adapting to change. It is an audacious idea and has long been an unpopular one, at the top and the centre of today’s health systems, where big stuff converges. But its implementation has been shown to be tractable and can be and is being made to happen. Its dissemination has started at little and local scale, in small ways, in small jurisdictions, albeit some now involving large-scale industries and whole health economies. Big ideas for little locations–little downside risk and big upside potential.
Realization of Information Policy Goals
The universal computer of Alan Turing (1912–54) and the lambda calculus of and Alonzo Church (1903–95) established strong mathematical foundations for computer science that have been extended and clarified but not supplanted. The technologies of machines and their handling of data and algorithms have been in continuous and exploratory coevolution over many decades–new devices, new applications, trial and error, compromise and optimization. Very much an art of the possible. Theory into practice and practice into theory. Information systems today reflect organic pathophysiology. Software systems have been characterized as following a progressive downward spiral of entropy accumulation and disorder, only revivable by periodic ‘binning’ and reinvention. There is all manner of systemic computational disorder lurking inside polished and admired machine-rooms and Cloud data centres, And the cyber mafia know it and exploit it! The e-passport gates in UK airports all broke down for twenty-four hours, three days ago as I write.
Substantial information systems have been constructed on what proved to be rapidly shifting sands of user requirements and available technologies. Over time, many have just about been kept operational and generating revenue, being firmly ensconced in place, and difficult to displace. They have struggled to accommodate ever-changing aspirations and expectations of their users, comprised as they were with inflexible and increasingly obsolete and unsustainable devices and software, held together over time by software patches. Their minders have had little choice but to palliate the malady, which is mostly incurable, for reasons of cost, complexity and logistics of cure. The skills and resources used by the programmers who wrote the original code may no longer have been around. To the outside world, the accumulating incapacity of such systems to perform is obvious, but it evidences an unrevealed pathology. The user has little option but to bear the burden imposed.
Set within these multiple contexts, the serially repetitive boom and bust of five decades of centrally mandated health care information policy, as tracked in Chapter Seven, is a sorry but understandable story. Figure 8.5 shows a diagram I constructed as part of my effort of those times, to give a more positive and helpful perspective on how to promote progress, contain and manage the inevitable impediments encountered along the way, and learn how to do things better.
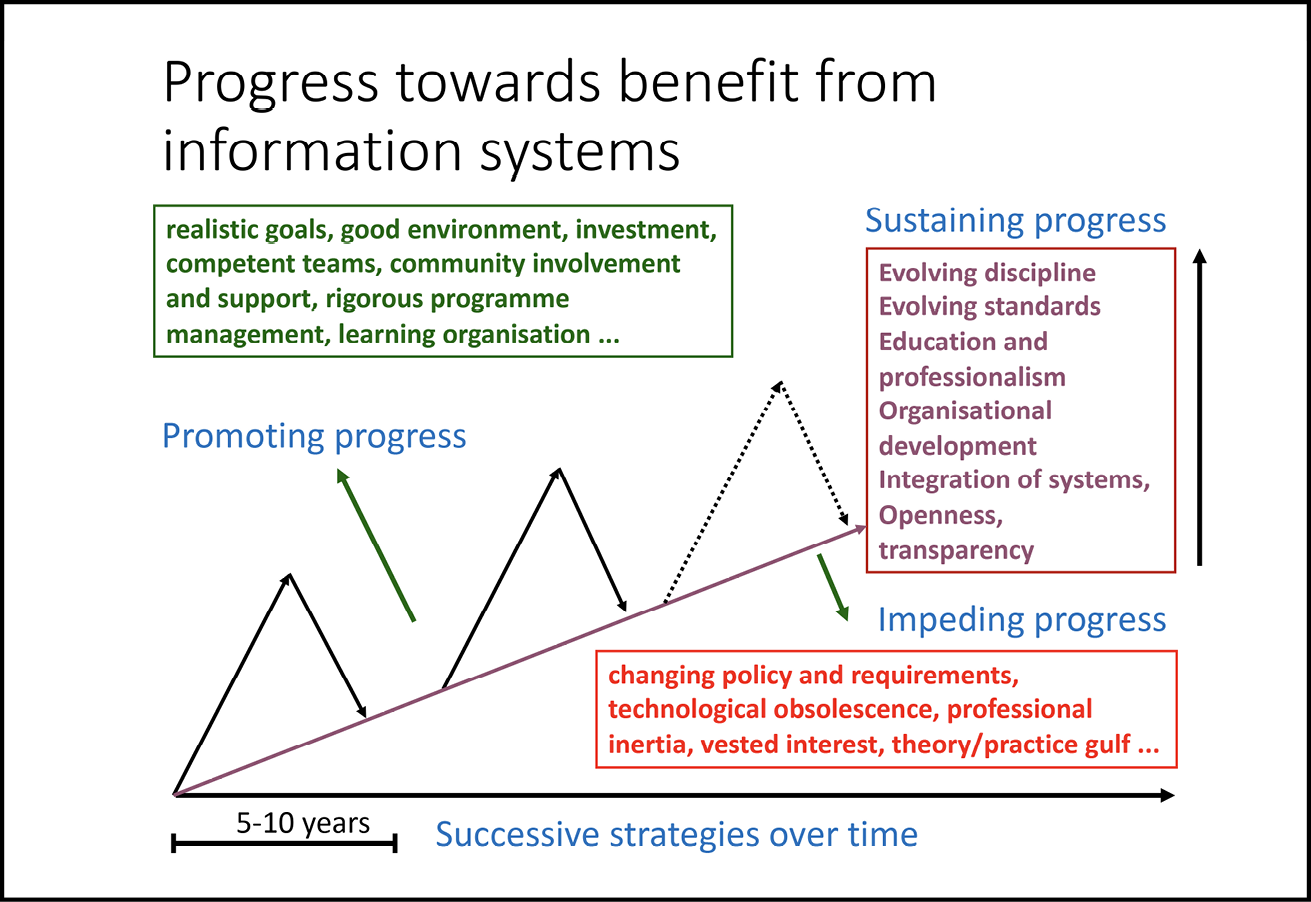
Fig. 8.5 Factors impacting on progress with health care information systems. The sawtooth progression of implementation of information policy–the gradient of improvement, overall, a matter of perspective and debate. Image created by David Ingram (2003), CC BY-NC.

Attendance and participation in many, both local and national activities and events, over many years, confirmed a dearth of motivated and supported communities and environments, near to the ground, in which coherent and useful and sustainable information infrastructure and utility could germinate and grow. The sawtooth of policy initiatives cut through services in those decades and was, at times, brutal, wasteful, costly and largely ineffective. The song about the Grand Old Duke of York and his ten thousand men comes to mind–marching his troops up and down the hill, the top being the summit of central policy aspiration and the bottom the ground level reality of local implementation, often leaving the troops half way in between, experiencing neither one nor the other!
The Portbou railway station process, extending or contracting the separation of wheels on carriage axles and attaching a new locomotive, to enable trains to operate between French and Spanish gauge railway systems, is played out for every train and every elaborately constructed axle, suspension and carriage. We observed it from our friend’s flat, which overlooked the railway, one way, and the sea, the other. This sort of process plays out, analogously, in standards conversion of information flow within and between information systems. The railway gauge conversion is rather exact–otherwise the train will not work. The information conversion is less sure and potentially riskier, when translating language and mapping information that is modelled differently throughout the system on either side.
The integration of data that preserves semantic integrity between different specialist domains of use has been a continuing problem in succeeding eras of IT systems for health care. It results in uncommunicating silos of data, limiting their utility and magnifying their cost and associated operational burden. It leads to lock-in between buyers and sellers of systems, with intended market competition tending towards monopoly. It limits meaningful dialogue between user and supplier domains. Health care professionals and other users of systems struggle to engage with developers and suppliers of the systems needed for their everyday work. Integration of systems, which require communication between different sectors and specialisms of health care, is impeded when they embody incompatible methods and technologies.
The original innovators of hospital information systems fifty years ago had to build locally bespoke infrastructure before they could create clinical applications, and such applications were, thus, typically limited to working within this local framework. Local application developers today must match their work to local definitions of data and workflows that are specified in terms of locally adopted and implemented infrastructure. Folding new scientific methods–for example involving genomics data or machine intelligence–into these databases and software workflows becomes a very laborious and time-consuming task–often prohibitively so. Aligning to a common, semantically attuned methodology that guarantees implementation within a common platform technology of infrastructure will multiply market opportunity and efficiency for the supplier of systems and increase the flexibility and choice of the user. And information utility all around will benefit and multiply. That is the necessary direction in which we must now shape care information utility. It is not, of itself, sufficient–other aspects of environment, leadership and governance will be central to success, as further discussed in Chapter Nine.
Designers of algorithms and users who capture and use data are now, increasingly, co-creators of programs. The World Wide Web has transformed the computational environment in which these programs are hosted and can connect. We have moved from an era where most of new project money was spent in creating local infrastructures. These progressed from central mainframe set ups to local area networks (LANs) and dial-in external telephone connections, linking users, machines and applications, and running in bespoke fashion on bespoke systems. We now have hugely more powerful machines, more extensive data stores and more connected networks. This enables architects, designers and programmers of systems to plug and play within network utility, processor and data store utility, and applications platform utility, drawing on substantially evolved software coding stacks and system development platforms. These all contribute towards enabling and causing what was previously complex and difficult to engage with infrastructure to disappear from view, subsumed within everyday information utility.
But much of health care data, today, still does not move through algorithms in ways that respect and reflect their semantics, standardized in ways that signify what they mean and how they can and should be safely and reliably used. In this arena of standardization, the focus of information utility will move to the frontline of health care services–to integrate with the wholeness of needs and attributes of citizens and the professionals and services they draw on and interact with. We have not yet envisioned and enabled a landscape in which that kind of utility can emerge and integrate–locally and globally, and safely–as it needs to do. But we have the tools to help us, and we have examples–used, improved, scaled and internationally adopted and standardized, in practice, showing that we are perhaps already halfway there.
Individual academics are used to defining their information system needs and methods. In their research, they capture and analyze data, build mathematical and computational models, communicate within teams and communities, and access libraries. They customize a personal information utility and infrastructure from shared resources, accessible wherever they are situated. In education, teachers and students interact through the learning resources and platforms used for their teaching and assessment. Some unique to each teacher and student and some shared within wider communities. Both teacher and student can customize and share.
The widely ramifying landscape of health care practice encompasses service, education and research. It extends more widely across the public domain in many kinds of professional and operational connections with management, governance, regulation and law. Health care professionals share this environment within their own and co-working teams, and with those they care for. All parties contribute to and use the underpinning information utility thus constituted. What data means is crucial to these connections and dialogues. And no one has time or inclination to work within multiple different infrastructures and multiple expressions of the same information within different information utilities.
Organizations everywhere have struggled with increasing information entropy, as the many hundreds of progressively obsolete, disjoint systems operating in individual centres of excellence attests. Here, it is the cost and effort of keeping workflow and records in good order that is the worry. Blackford Middleton’s team’s estimate, many years ago, of eighty billion dollars per annum of consequential cost arising from the disorder in health care information in the USA, even if only very approximate, was indicative of the scale of problem this presents. The addition of personal genomics data to care records, rendering them intrinsically beyond anonymization, adds new technical, logistical, legal and ethical complexity to the challenge. Integrating the burgeoning range of home-based information appliances, to underpin the effectiveness and safety of self-care and hospital-at-home, presents further challenges.
As the world has faced choices in moving to standardization of technology, it faces choices about the semantics of data, not just at the level of terminology and description, but in its clinical context and meaning. This has moved standardization of care records into the realm pioneered by openEHR, in creating and exploring common ground on which to build sound and sustainable semantic interoperability and integration of care records. This has been an uphill quest of thirty years, to develop and implement capability for expressing and communicating the requirements of this coming era of care records, and innovate–clinically, technically and organizationally–to experiment with their implementation as a common ground of care information utility.
We need a utility that captures and communicates the semantics of the data, connects the algorithms that process the data, and makes all the information safely accessible and available for patients and professionals, anywhere, anytime, in their consultations and interactions. We need a utility that does not embody monopoly and respects ethical and legal rights and responsibilities of all participants. We need a trusted utility tuned to continuous, effective, efficient and safe updates and changes, engaging innovation within worldwide community of users and providers of systems–from industry, academia, public and voluntary sectors alike, under trusted governance. The information utility we need will be operable across Cloud and wristwatch, meeting the needs of all its users and organizations. It will provide a common method for integration of the detail and context of health care information, but not be a sole or exclusive engine in implementing these. There will be specialized engines of integration and innovation for research and education. There will be algorithms that are shared, just as physicists unravelling symmetries of particle physics share computational methods.
Governments have focused on painting a picture of what a more smoothly functioning and effective health care information world might look like. As preceding chapters have shown, the grand challenges of data and records remain stated very much as they were fifty years ago, although hundreds of billions of dollars are spent annually on systems that do not yet rise to the challenges then set. Of course, they can show the shiny car bonnets and souped-up engines of today’s giants, but these are not on a path to the information utility that is needed, because many commercial interests fear loss of power and revenue if their markets become vendor neutral, and publicly owned and governed information utility and tooling come into contention. New players would, they quite reasonably fear, then more readily and reliably innovate to compete with the well-established, because the new ecosystem of common ground, on which all systems could be based, would enable them to bypass much of the current prohibitive cost of market entry. They would, moreover, have the benefit of a clean slate in adopting the more efficient and agile development tools of today.
But without this common ground, there can be no commonality or community of practice in future care information utility. If achieved, it will simplify systems and enable much more affordable, efficient, effective, safe and useful information resources. Mathematicians support one another by sharing their methods and insights, and thereby mathematics benefits, and indirectly so does society through the science and practice that mathematics underpins and enables. Information utility will likewise rest on commonality and open sharing of method, governance and community of practice. I have given the information utility for health care an acronym, CIU. I invented openEHR as a name and brand that caught on, but who knows whether this might too. CIU and uic, perhaps. Care Information Utility (CIU) with you in charge (uic), placed, owned and governed in the commons of the public domain.
We now need a new community of information architects to bring all this to life, in the spirit of Fred Brooks’s advice about systems needing architects. Architects to imagine and lead the building of the CIU. Charles Moore (1925–93), the American architect credited as the founder of postmodernism in architecture, emphasized architecture as an instrument of connection, as a medium to reflect human experience, where occupants must be able to imprint their lives on a building. Norman Foster, the English architect, described architecture as an expression of values, saying the way we build is a reflection of how we live. Information architects are needed to illuminate and lead the way in support of human, not machine, reinvention of health care for the Information Society.
This is certainly an audacious idea and maybe a bit too hopeful! But if pessimists doubt its realism, the default fragmented alternative is far less hopeful to contemplate. Its purpose and goal is a better and sustainable CIU. It requires grounding in new ideas–about co-creation and custodianship of records, citizen and professional relationships, software architecture and ecosystem standardization, and governance. It must be built on common ground that instills hope and belief in local communities on the ground, where there is, today, much pessimism. Hubristic pretention toned down into a more capable, realistic and humble approach. Hope and pessimism finding common ground in shared creative endeavours, of the kind and quality shown by the outstanding pioneers celebrated in the next section.
Pioneers of Health Information Systems
My songline has seen some seven eras of NHS national strategies to bring health care services into the Information Age: each replaying a common theme saying why it was needed and promising what would be achieved; each conditioned by prevailing socio-technical attractions and distractions of the times; each dependent on new national proponents and leadership; and all too quickly, mostly running into sand. It would be a task of Sisyphus to catalogue in detail the many pioneering efforts to do these things better that I have observed and participated in during my career. It would be too long and much of it would now be uninteresting and irrelevant. There are other places to dip into this history. The IMIA Yearbook of Medical Informatics journal, edited by Jan van Bemmel, kept pace for many years, as do the MedInfo publications (conference proceedings from the World Congress on Medical and Health Informatics) and HIMSS (Healthcare Information and Management Systems Society) publications of today, and specialist journals.
My aim, here, is to introduce several amazing pioneers who have been inspirational for me, and whose ideas and contributions have been foundational to how I have come to envisage the nature of the future care information utility, and work collaboratively and internationally, in the public domain, to create the methodology, communities and governance this will require. I describe how they have connected with me along my songline, some very close, and some far away, and the wide impacts they have had. They are contrasting stories of struggle to create the future, seeking to make and do things that will count, and each illustrating different facets of grand challenge and wicked problem, in what they undertook and accomplished.
Octo Barnett–Massachusetts General Hospital and the MUMPS Language
Fig. 8.6 Octo Barnett–clinical and computer science pioneer of medical informatics at the Massachusetts General Hospital and Harvard University. CC BY-NC.
I met Octo Barnett (1930–2020) in his office at Massachusetts General Hospital in the early 1980s and spent the day with him. He was a foremost and celebrated pioneer of his times.32 It was an honour to spend time with him at that still formative stage of my career in health informatics, much as it had been with Arthur Guyton, a decade before, at his laboratory in Jackson, Mississippi, as recounted in Chapter Four.
Octo knew of my work at St Bartholomew’s Hospital (Bart’s) with John Dickinson and asked to receive a copy of the Mac Series MacMan model of cardiovascular dynamics. He was already a legendary figure in medical informatics and was also active in curriculum change in medical education, linking informatics with the New Pathways Programme at Harvard University. He had been following the graduate entry programme and curriculum innovation at McMaster University, a few hundred miles north of Boston, and I flew there from Toronto to meet him.
Octo immediately impressed with his energy and enthusiasm; his work was an all-consuming passion. Harvard made him a professor in both medicine and computer science, in recognition of these twin motivations and driving forces. Along with Homer Warner (1911–2012), at Salt Lake City in Utah, he was a polymath who took the fledgling computer by the scruff of the neck to do his bidding. In the DxPlain system, he and Edward Hoffer took medicine by the scruff of the neck, to shoehorn diagnosis into a paradigm of decision support, mapping from the symptoms, signs and measurements of clinical practice to a guided pathway for diagnosis.33 In his earlier work centred on computerizing medical records, he learned the practical implications of implementing the requirements for assembling a clinical record, incrementally over time and accommodating the sparse, dynamically changing structure and occupancy of the data collected. These proved extremely difficult to represent and manage efficiently and effectively, using the database paradigms of the era.
Faced with this reality, and displaying great imagination, he worked with Neil Pappalardo and others to create the Massachusetts General Hospital Utility Multi-Programming System (MUMPS) language, with its ground-breaking innovation in data storage and retrieval, integrated seamlessly and efficiently with computation. The MUMPS language was a key that opened doors to practical applications that have persisted to this day, in leading medical record and patient administration systems and, more widely, in financial transaction processing systems. The functionality that their innovation squeezed from the minicomputers and operating systems of the times, was astonishing. The MUMPS language became an international standard. It was a pragmatic and interpretive language, well suited to both its clinical and early technical contexts, and it performed extremely well.
Through the decades from the 1970s, computer science struggled with formal database architecture, going through a long circle dominated by the mathematical formalism of relational database theory, and then gradually back towards simpler, MUMPS-like key-value stores. This evolution tracked transition into the Internet era of networked systems and the need for datastores to accommodate a greater variety of datatypes, of different shapes and sizes, at much greater scale, increasingly less suited to implementations of the relational model.
Programming languages evolved along two principal lines of formalism. A culture war developed between adherents of object-orientation, centred on rigorous representation of data structure, and adherents of functional programming, centred on rigorous representation of algorithm. In the object-oriented scenario, processing of data was incorporated through methods attached to descriptions of the data on which they operated. Functional programming was the idyl of computer scientists concerned with specification of rigorous and provably correct programs. In this scenario, description of data was integral with the scope of the program language. Each paradigm struggled with the other’s principal concerns. Niklaus Wirth’s pithy description that ‘Algorithms + Data Structures = Programs’ held in both domains of formalism, of course. Over time, functional programming languages improved their capabilities with respect to diverse datatypes. The pragmatic world of FORTRAN continued to hold sway in scientific programming, where datasets were more orderly and there was less concern about theory of computation! Greater formality and problem domain specificity arose in languages like ALGOL, PL/1, APL and Simula.
At our meeting, Octo promised to send me the source code in MUMPS of some of the decision support and educational software he had devised with Edward Hoffer, including one that related to my own work in modelling clinical physiology. This guided doctors in managing fluid and electrolyte balance for acutely ill patients.34 I wanted to see how this might fit within the computer-based learning software platform that John Dickinson, Khursheed Ahmed (our colleague and friend at McMaster) and I were developing (MacAid).35
MUMPS code is dense and parsimonious. One of its principal goals was to use data storage efficiently, in handling the very sparsely populated arrays of data which are characteristic of the clinical domain. Another was to fit the program into the smallest possible amount of main memory of the minicomputer on which it ran, so that the programs of more users could be accommodated, simultaneously. The logic embodied in voluminous and rambling code can be hard to understand, and so, too, can be that of parsimonious code, but for different reasons. Algorithms can be artfully subtle, rather as mathematical proof can be. And where descriptors of program variables and processing operations are kept brief, and thereby the length and number of lines of code kept as small as possible, they can be difficult to read and understand.
Octo and his team became past masters of this parsimonious art and, as with many geniuses, had little regard for the reader of lesser brain, seeking to understand their code! To my eyes, it combined all manner of detailed medical knowledge and data, with program logic reasoning about them, in a rather haphazard way. The program that I analyzed was both a database and knowledge base of the specific domain of fluid therapy. To update this program with changing clinical understanding and practice, would have required understanding not just of the logic, but also of the knowledge and data it was based on at the time, and how it reasoned with them. This looked to be of doubtful sustainability, and so it was proved.
Here, in about 1980, I saw the growing need to separate concerns of data, algorithm, knowledge and reasoning, if software for the field was to prove sustainable beyond the insights and expertise of its pioneers. Another difficulty that started to emerge was a loss of access to the skills and knowledge underpinning the software. Attrition of effort–because of rapid obsolescence of clinical domain knowledge and requirement, available technology and knowledge and skills possessed by program developers–became a significant factor limiting progress in this era of transition.
COBOL (Common Business-Oriented Language) was a hugely successful development for business data processing of those times. Many applications written in COBOL cost many millions of dollars and required much time and effort, to create. They continued to perform essential roles, but, over time, it became increasingly impractical to assemble the machine environment and technical skills needed to adapt them further. They continued as historical artefacts, deployed within newer software ecosystems as binary modules that did what they said on the tin, but could not be changed. This reality may not have been apparent to purchasers, who then receive a painful awakening should their needs not be met in practice, requiring the module to be changed. This occurred, for example, when software was purchased for a major NHS IT project, where a demographics module managing patient details needed to be changed to match UK practice. These considerations arise more widely where obsolete tools and methods render impractical the incremental development of software over long periods of time.
The evolution of methods whereby systems can, more easily and sustainably, be integrated one with another–customized and localized to suit different practice in the user communities served, and updated as science and practical requirements change–is a considerable challenge. One that my involvement with care record architecture has continued to face, since those times.
Jo Milan–Royal Marsden Hospital and Tertiary Cancer Care
Fig. 8.7 Jo Milan–architect, designer and implementer of the innovative hospital information and care records ecosystem of the Royal Marsden Hospital, London. CC BY-NC.
If ever there was a person who most completely and powerfully epitomized Denis de Rougement’s characterization of the necessary synthesis of head, hand and heart, in his 1936 book Penser avec les mains [To think with the hands], that person, for me, would be Jo Milan (1942–2018).36 Sadly, Jo died from sepsis in late 2018, just as my wife was battling for her own life in intensive care. Jo was my hugely talented and committed friend. He is greatly missed. In temperament and pragmatic mien, he, as physicist computer scientist, and Octo, as clinician computer scientist, were quite alike.
I met Jo in the early 1970s, when we were both appointed to the relatively new Computer Topic Group of the UK Hospital Physicists’ Association. Also there, I first met Christopher Taylor. Chris was using the computer to analyze shapes of cells in microscope images of pathology specimens, to complement the trained eye of the pathology laboratory team. Jo was completing his PhD based on pioneering work to computerize the collection and display of ultrasound images, having created the early Rad-8 radiotherapy treatment planning software some years before. I have written of his pioneering work in medical physics of the era, in Chapter Seven. Here I focus on his contribution as architect of the hospital information systems for the Royal Marsden Trust specialist cancer hospital in London. There is a chapter devoted to this story in the medical oncologist Eve Wiltshaw’s history of the Royal Marsden.37 She was one of his close clinical supporters there.
The Marsden has long been preeminent in science and cancer research, with its connected Institute of Cancer Research. Its information systems enabled and underpinned synergism between clinical service and research. It is, I think, no exaggeration to say that Jo was a cornerstone contributor to the Marsden’s pre-eminence, nationally and internationally, as Wiltshaw’s book affirms. His massive achievements exemplified good information utility–at the Marsden it worked and flowed and was, in Birnbaum style, substantially invisible. That is, to all but those, like his team and some, like me, among their wider admirers, who knew from whom it came, how it was achieved and the effort it involved.
Jo and I kept in close touch as we progressed through our respective careers. In the mid-1970s, Jo was taking first steps in computerizing the Marsden’s information systems. His work on this was conceived, designed, implemented and operated in-house, serving the two sites of the Marsden–one in Sutton, twenty miles from the centre of London, and one on Fulham Road, in central London. Jo worked at the Marsden for the rest of his professional career. He built a loyal and respectful team around him, led them, and supported them. He met and married Sarah, there, and they became family together, and work colleagues, for life–an impressive achievement in itself!
Jo was the most practical of physicists and engineers, whose intellectual life was everyday spent exploring ideas, devices, methods and systems. In later years he was busy making and flying autonomous model airplanes and machining novel kinds of engine, which he discussed with me at length in evening phone calls. Mine are personal reflections on someone who was the most authentic, motivated, diligent and talented of people and friends. He was not at all a saintly figure–he was crusty, emotional, dogged and straight as a die. He argued and disagreed a lot, but only in pursuit of his truth and goals. In the proper sense of the words, Jo collaborated and cooperated. In the words of one of his long-term colleagues, who told me of Jo’s untimely death, when we met at an openEHR Foundation meeting in London: he was a boss respected because everyone in the team knew there was no task that he asked them to tackle that Jo himself was not equipped to tackle better!
Jo started to think about the design of an integrated information system for the Trust, in the multiple contexts of operational management, clinical service and research. At a leading institution like the Marsden, clinical service and research are closely aligned. Clinicians at the Marsden were focused on exploring and describing the time course of innovative treatments and their everyday practice was on the frontiers of research. Cancer was a cause of death at all ages, and experiment in its treatment was essential, albeit carrying risks of its own. In cancer treatment of that era, efforts were devoted to novel methods of surgical excision, radiotherapy and many new compounds and combinations of compounds, that might slow, reverse and eliminate tumour growth.
In a sense, every patient was to an extent being treated experimentally, and was thus a candidate, if consent was given, for inclusion in clinical trials. These are scientific experiments to test the safety and efficacy of new drugs and drug combinations. They are the gold standard whereby new interventions are permitted and regulated for widescale use in clinical services. Clinical trial data and its analysis formed a key plank of medical statistics discipline. Clear protocol for conduct of a trial, definition of the data collected, and analysis of results, was required for ethical approval of experiments involving tests in animals, human volunteers and patients.
Clinical research has long relied on separate information infrastructure from that provided for clinical practice because of the need to record structured, longitudinal data on interventions and outcomes. The hospital focus was mainly on its clinical records and management information system, but a separate clinical research management system was needed to enable clinicians to collect and analzse structured clinical research and trials data for their particular specialties. From the outset, Jo was anxious to avoid duplication of effort by ensuring that, wherever possible, routinely collected clinical data should be made available to the clinical research databases. He envisaged the hospital information system throughout as in need of a coherent and common unifying thread of information. Living every working day as a citizen of that community, he knew this requirement intimately. As a physicist and engineer, he possessed a mind trained and supremely competent in formulating a coherent and consistent model of that information, and the interrelationships of roles and activities represented in all its components–about wards, outpatient departments, diagnostic and therapeutic support services, pharmacy and so on–and in workflow and management, at department and Trust levels, bringing it all together.
Jo knew this world better than any external agency ever could, given whatever resources and deploying whatever skills. He tolerated no blandishments to the contrary. That often meant that ninety percent of the wider world was already against him! Fortunately, under the umbrella of hospital physics discipline, itself used to adopting a defensive encirclement of its right and need to exist in practical everyday hospital context, he was sponsored and supported to explore and discover where his interest and insight might take him. He and his team created and sustained a unified information system. Jo was its Fred Brooks-style architect. My colleague Steve Pizer was a colleague of Brooks at University of North Carolina (UNC) at Chapel Hill. He and Jo introduced me to the insights of Brooks’s book, The Mythical Man-Month.38 In the early days of MUMPS, Jo became expert in framing his ideas within MUMPS code, and in design and procurement of the computer system, network and user devices.
The team sustained and evolved an operational system for the Trust, through successive, roughly seven-year cycles of new generations of design and implementation, while hardware and software technologies and standards underwent a Moore’s law pattern of rapid change and extension.39 They explored a combination of MUMPS and relational database formalisms for persisting their data model and confronted the major issues impacting system performance that were becoming clearer in those times, where optimization of speed and depth of access into complex and diverse individual patient data structures conflicted with performance in searches across all patients and activities. They introduced, in parallel, a database containing just a time-sequenced index of all activities, which, in combination with the full database, solved this performance problem and transformed the system’s capabilities. They combined data and programming code in a dictionary of data objects, mirroring the rising object-oriented paradigm of the era. This transformed the functionality and flexibility of the system and reduced the development time and maintenance burden it imposed.
Jo thought through the place of standard terminology, first in relation to the classifications offered by the Systematized Nomenclature of Pathology (SNOP) and the Systematized Nomenclature of Medicine (SNOMED) for pathology of tumours. He used them when he had a use and positioned them where they were useful. He became an early master of the spreadsheet and integrated a spreadsheet module within the analytical functions required for management reporting purposes. His system dealt with almost all aspects of the activities and costs of the Trust, save for the accounts, payroll, estates and personnel functions.
I wrote in Chapter Five of one striking example where the coherent design methodology of the Marsden system shone. This was in the vetting of the system for Year 2000 vulnerability–a central edict of the NHS at the time was that such a detailed review be conducted. Jo shrugged his shoulders, saying he knew the answer before looking but had to go through the hoops and write a report. What the design of the Marsden system enabled him to verify in seconds–because time computation was carried out throughout by just one tiny, shared object module–required many months of team effort in assessing other less-ordered spaghetti heaps of code, where time computation and other common functions were coded, repetitively, in a multitude of long forgotten places within the programs. A situation sadly typical of many information infrastructures, still, today, and a key reason for the repeating heavy cost and burden on services, of the efforts to improve health information infrastructure more widely.
When I switched from the domain of mathematical modelling of body systems and computer-assisted learning into that of health information architecture, in 1990, Jo and I developed closer working links. Jo was a great mentor and support to me. When he struggled with sustaining and extending his pioneering work at the Marsden, against the management predilection of the times to buy in or outsource IT systems and services (and thereby seeking to avoid the pains experienced in devising and growing local solutions), I helped him through some tough months.
I was working at that time, on getting the GEHR (Good European Health Record) project team into good shape, with Sam Heard commuting several months a year from Australia and me establishing my first academic group, linking clinical skills and informatics at Bart’s. In his work, Jo recognized, pragmatically, that patient notes were so widely varied and idiosyncratic, and in many aspects necessarily so, as to defy the sort of information model that was state of the art in those times. He came alongside in the GEHR project and was a great litmus test and mentor of its evolving ideas and progress. In these debates, the separation of information model and data model came into clearer focus. I remember with pleasure him attending the founding dinner of the project where the GEHR partners and the leadership of Bart’s sat down together in Dean Lesley Rees’s (1942–2022) elegant dining room at Charterhouse Square. Jo was opposite Sam Heard and I gave a speech, sitting with Dean and health authority chairs and Alain Maskens, who, with Sam, had been a leading light in drawing together the GEHR Consortium bid and inviting me in to take the lead. Remembering the powerfully argued debates between Sam and Jo about clinical requirements and relational modelling of data in the form of tables, one the dominant clinician, one the dominant engineer, and both versed in the domain of practice that joined them, I had a good ‘in joke’ to tell, celebrating their close relationship across a table! I can still see my mind’s image of them high-fiving across the table!
Through Jo, I first met Thomas Beale, a young Australian IT consultant living in England at the time, in 1992. Thomas was developing his skills in using the evolving World Wide Web and building a career in software design and object-oriented programming, well versed in the object-orientation mission of Bertrand Meyer. Jo had employed him as a consultant at the Marsden and these two great minds had already engaged one another, to their mutual enlightenment, I think. Jo, ever the pragmatist, believed that his highly innovative ETHOS higher order software brainchild, running on the two sites of the Marsden, gave the best of object-orientation, flexibility of MUMPS programming and rigour of relational database persistence of data.
At that time, I needed to establish a new paradigm for the GEHR project, for how it conceived and expressed its mission to create a formal architecture for electronic health records, as discussed more fully in Chapter Eight and a Half. This was to be central to how we would subsequently enact the exploratory work and build teamwork and environment around it. It was a formidable consortium, comprising different expertise and interests from clinical professional, technical and organizational management backgrounds, working in academia, small and large industries, and health care organizations. I recruited Thomas as a disrupter, to help with new ways of thinking. I wanted him to bring his knowledge of object-orientation into the mix of methods under consideration. I did not appreciate at the time quite how good and well-adapted he would prove in that role! If I were doing the same today, I would bring a functional programming disruptor to the table–I know just the one!
It was a risky but necessary strategy and felt quite threatening to some, challenging already established teams and relationships within the consortium membership. As described further in Chapter Eight and a Half, I managed to create and sustain a cohesive and committed team through some very difficult years, initially anchored by our physical presence with Sam’s colleagues, Mel Salkind and then Lesley Southgate, and the Primary Care Department she led, and my newly conferred professorial status in the Medical School. Also, supported by a superb administrative assistant, Marcia Jacks, who had built her career first as a secretary to the head of Primary Care, then as a departmental manager for me when we later moved to establish the (CHIME) at UCL, and finally as divisional manager for Ian Jacobs’s Institute for Women’s Health within UCL Biomedicine.
On the completion of the GEHR project, we were facing key issues of how to progress from the GEHR information model to a new care record architecture based on what we started to call two-level modelling. The term described a methodology yet to be realized. The first level was focused on creating clinician-defined and governed ecosystems of care records, containing all kinds and varieties of clinical data, composed from and conformant with a single generic pattern of clinical data model, customizable according to both clinical discipline and local organizational requirements. The next level was focused on the design of a common and openly specified software platform infrastructure, to host and enable free flow of the content of care records structured in this way, within and between systems designed to generate, store, communicate, process and interrogate these records, to support bespoke and specialist health care domains and purposes. The purposes served and the manner they were addressed were thus to be wholly in pursuit and support of the needs of clinical services, including those to be operated by patients and citizens, themselves, and, likewise, the needs of clinical professionals and their health care organizations. The care record ecosystem needed to be configurable according to local needs, with data structures standardized according to clinically determined patterns, and the specification of the platform for hosting these data kept neutral with respect to its underpinning implementation technologies and suppliers.
This was the new endeavour on which we set to work–Sam and Thomas pursuing a commercial pathway in Australia, setting up Ocean Informatics (now Ocean Health Systems), and me, with Jo and Dipak Kalra, joining forces in the mid-1990s, with Jane Grimson and Bill Grimson, in Dublin, and other partners, to collaborate on the Synapses project. Jo and I devised and wrote the work package that captured this new architecture, expressed through the concept of a clinical object dictionary. Sam and Thomas, in parallel, evolved a very similar idea and christened it an archetype repository. In the subsequent years, these worlds recombined and the rest, as they say, is history–the history of GEHR and openEHR that I tell in Chapter Eight and a Half.
I turn, here, to highlight another highly significant period some twenty years after I first met Jo, and to the report prepared by the National Audit Commission in 2003–04, appraising progress of information infrastructure for the country’s ninety-three Acute Hospital Trusts. Jo provided me with the content relating to the Royal Marsden Hospital, which I draw from here. The report focused on the contribution of information systems to the clinical work of these Trusts. It explored: extent of use; clinical value derived, as assessed by working clinicians; progress towards paperless operation; and value for money achieved. I have an original copy–it counts as an inukbook–its message is clear.
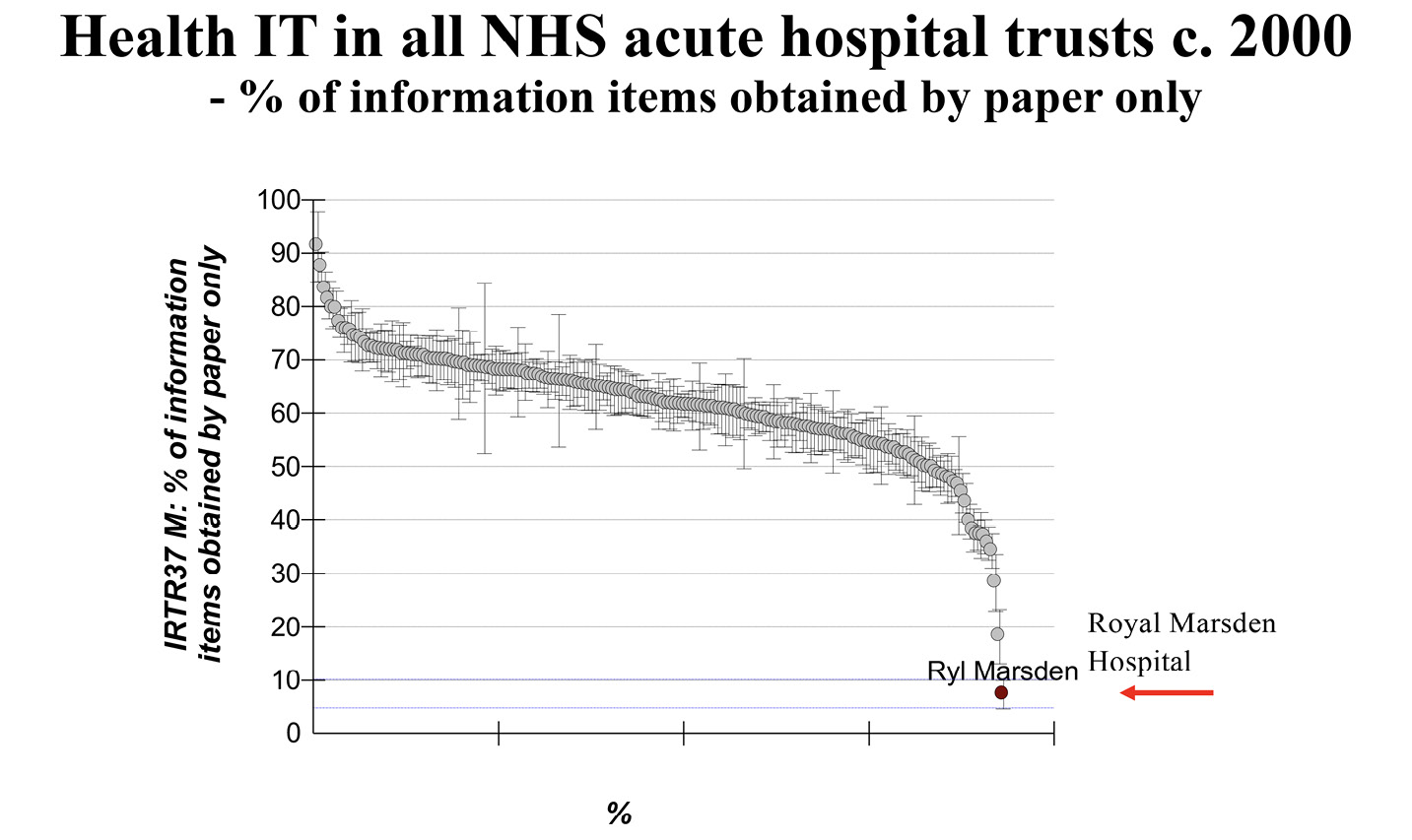
Fig. 8.8 Progress in going paperless: a figure illustrating the outstanding achievements of Jo Milan and his team at the Royal Marsden Hospital. Adapted from the 2003–04 Diagnostic Audit of NHS Acute Hospital Trust IT, The UK Audit Commission. Image created by David Ingram (2010), CC BY-NC.
A widely touted objective of the era was ‘going paperless’. It still is. The report chart from which Figure 8.8 is adapted shows the percentage of information collected only on paper on the ordinate and lays out the amount, Trust by Trust, from the one with the highest to the one with the lowest along the abscissa. Information gathered only on paper comprised less than ten percent of the total at the Royal Marsden. The next most paperless Trust had double this amount of paper-only information. The sigmoid curve is strikingly revealing. The median level of information collected on paper only was around sixty percent and the flat central region showed a range of thirty-five to seventy-five percent in almost all Trusts. The highest paper-only pile was over ninety percent. The Marsden is highlighted in red in the figure, as number ninety-three in the sequence of ninety-threeTrusts. As an example of how a picture can be worth a thousand words, this one could not be bettered!
Figure 8.9, also adapted from the report, shows relative value for money obtained–how well the Trusts were doing in obtaining value from their expenditure on information systems, in terms of the amount of information they gathered. Again, the ninety-three Trusts are charted, but in a new sequence, along the abscissa, and the score allocated to each, based on data from the Trusts, is shown on the ordinate, from the Trust achieving greatest value for money on the far left, towards those achieving progressively less value for money, Trust by Trust, along the abscissa. The red line is used to pinpoint the Marsden’s score–it is an extreme outlier in terms of value for money in eliciting information. The data are arranged with a score of zero at the median performing Trust.
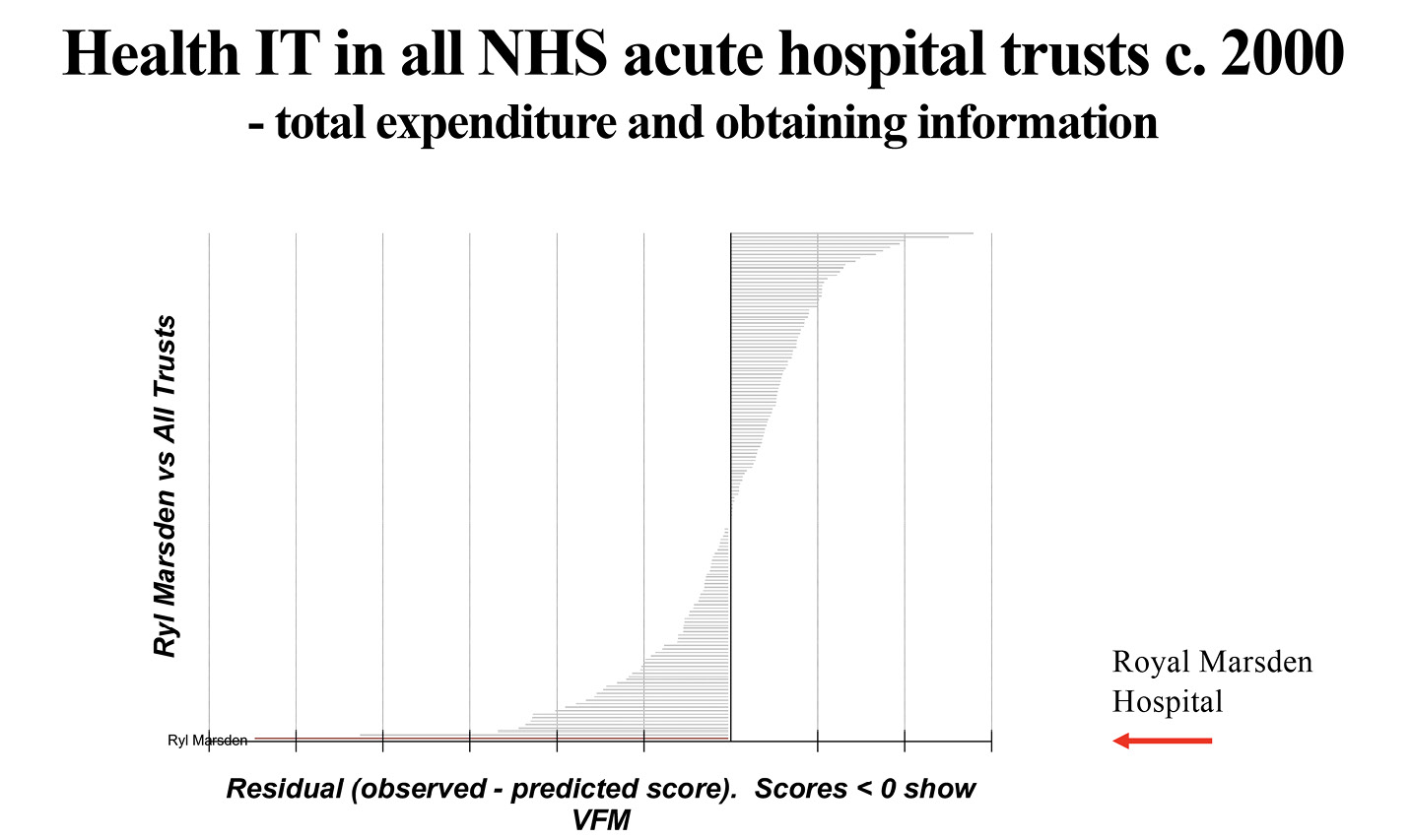
Fig. 8.9 Cost-benefit expressed as information acquired in relation to investment made, further illustrating the outstanding performance of the systems developed at the Royal Marsden Hospital. Adapted from the 2003–04 Diagnostic Audit of NHS Trust IT, The UK Audit Commission. Image created by David Ingram (2010), CC BY-NC.
Figure 8.10, also adapted from the report, is based on attitude surveys of staff in the Trusts about their use of the local information systems. Here, value for money is judged in terms of the ratings provided by Trust users, about their use of the systems and their assessment of the quality and relevance of the information for their work. Once again, a red line is drawn to position the Marsden. Once again, literally outstanding–that is extreme outlier.
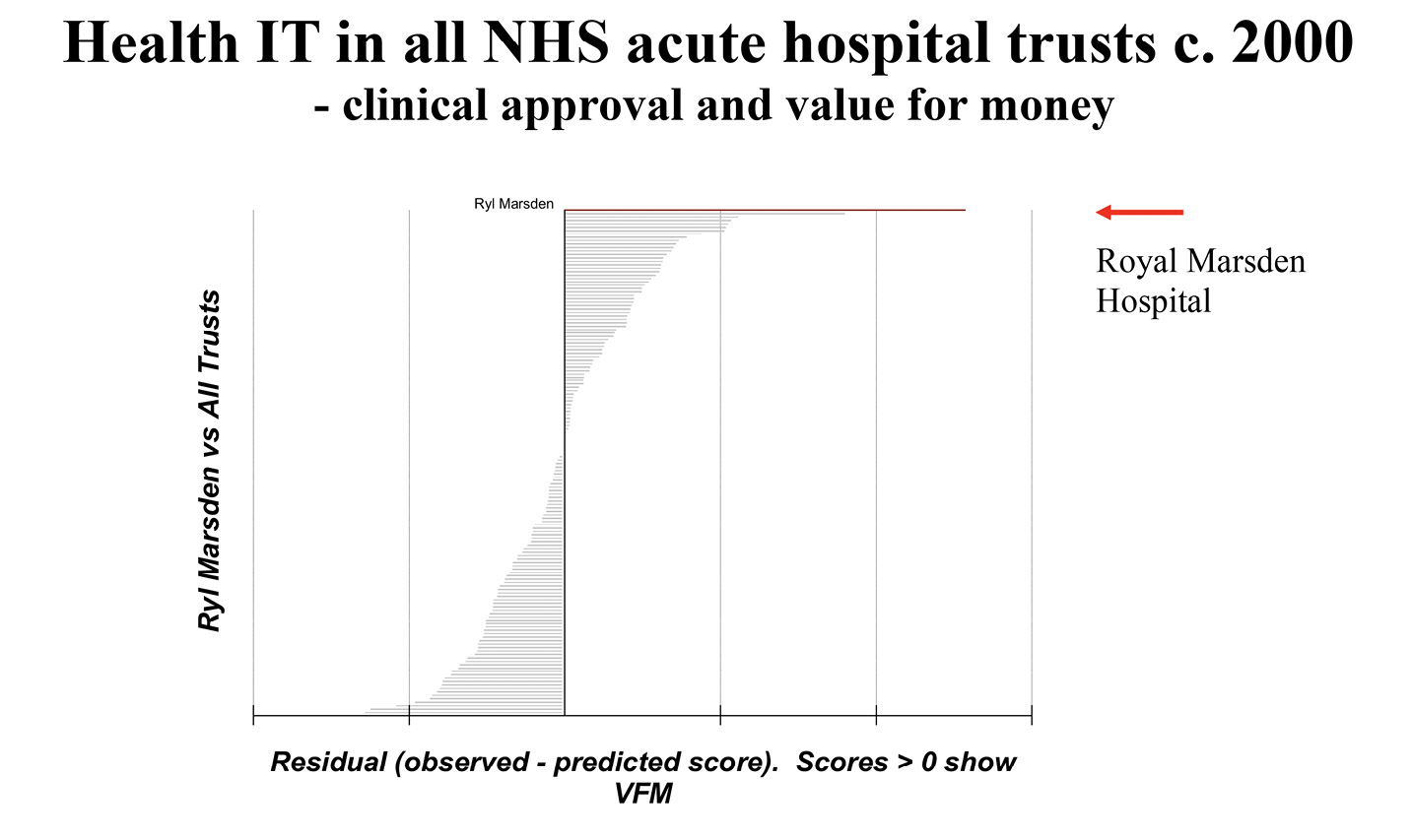
Fig. 8.10 Cost benefit expressed as clinical value perceived in relation to investment made. Illustrating how clinicians at the coal face of care rated the systems developed at the Royal Marsden. Adapted from the 2003–04 Diagnostic Audit of NHS Trust IT, The UK Audit Commission. Image created by David Ingram (2010), CC BY-NC.
Positioning individual cases within such distributions is a good way to express and learn from individual performance. It is useful and effective for good and bad performers alike, in their self-assessment, to take pride in achievement and motivate remedy and improvement of practice. There are important messages here for the wider community. They have largely gone unseen and unheard–not willfully but certainly neglectfully–which is, itself, significant. For me, these messages start and end with Jo Milan as a person–who he was, how he was perceived, how he achieved what he did, how the Marsden systems were designed, implemented and evolved, how they were managed, and how Jo himself was received and treated. He was a tough, highly-skilled and focused innovator–I found a lot of Jo in what I read of the engineers discussed by Samuel Smiles (1812–1904), who I wrote about in Chapter Five.
In a noisy world, a quietly pursued mission and modestly spoken words easily go undetected and unrecognized. It sometimes seems that experimental evidence of an outcome is required before the experiment is seen as credible or to be supported. In the commercial world of technology, innovation follows a cycle of hype–characterized by the Technology Foresight arm of the Gartner consultancy in the rise, fall and levelling off of the hype cycle. The hype diagrams sometimes look akin to a lightly damped and oscillating, controlled system, with changing target level and feedback signal! In a dazzling world, less visually lustrous images than those capturing Jo’s and his team’s achievements at the Marsden easily go unseen and unrecognized. And yet these are the hallmarks of the Birnbaum–best when least visible–information utility! In a competitive and argumentative world, some wish neither to hear, see or think about what they do not want to hear, see or think about. Jo’s achievement was monumental and heroic. At the Marsden, it was felt but not well recognized by its management team, probably focused more on key performance indicators directed upwards than to what was being achieved locally on the ground. Clinician support, as shown in the above graphs, was more understanding and supportive, as warmly evoked in Martin Gore’s (1951–2019) funeral oration for Jo, I gather, which was fulsome in praise and acknowledged that Jo’s contribution had not been duly recognized there. His fame spread abroad, but in the national NHS context he was largely overlooked. In Chapter Five, I gave examples of similar patterns in innovators and innovations of past centuries. Jo’s story ranks alongside them.
Stanley Huff–Intermountain Healthcare and Clinical Element Modelling

Fig. 8.11 Stanley Huff–career-long Chief Medical Informatics Officer at Intermountain Healthcare in Utah and architect of its innovative information systems based on clinical element models. CC BY-NC.
I mentioned Homer Warner, the doyen of medical informatics based at Salt Lake City in Utah, in my above profile of the pioneering contributions of Octo Barnett at the Massachusetts General Hospital and Harvard University in Boston, USA. Some of his early work from the 1970s that used a computer-based Bayesian statistical model for teaching clinical diagnosis, caught my eye. One of Warner’s academic progenies of the early 1980s was Stanley Huff, who worked over the following decades at Intermountain Healthcare, where he played a notably practical and clinically focused pioneering role in the evolution of its information systems, just as Octo did in Boston. Stan graduated in basic science before switching to medicine, in which he specialized in pathology. In the early 1980s, he worked for a while at Bell Labs before joining Intermountain for the next thirty-five years. An amazing pedigree of synergistic connections of science, IT and medicine!
The team and environment Stan created at Intermountain, and the information system it gave birth to, looked to bear some resemblance to those which Jo Milan created at the Royal Marsden Hospital, in and from the 1970s. Intermountain being a very considerably larger and more wide-ranging health care community, and Stan’s initiative being based on close industry partnership for the implementation of systems, they also differed considerably. At the heart of both their systems was a novel approach to rigorous separation of clinical data models from programs, in modelling and implementing a coherent and modular system architecture. The Royal Marsden advances were developed in the public domain. At Intermountain, the methods devised were developed in partnership with the corporate IT private sector.
As with Octo’s pioneering work in the creation of MUMPS, Stan’s foundational contribution in creating and shaping the Intermountain systems, as both clinician, architect and implementer, was iconic. I do not know how the relationships and associated intellectual property rights were handled in the commercial partnerships, but the general approach in such cases has necessarily been to anchor the IP protection under proprietary lock and key, integral with the contracts between the health care and industry partners. Wider generalization and dissemination of the Marsden systems was constrained by it not having the benefits that derive from a strong and synergistic industrial partnership. This proved impossible for Jo to secure within the UK health care IT markets of the times, and in the context of the subsequent tumultuous management of the contractual framework for procurement of systems for the NHS National Programme for IT.
I have known little of the inside story of Intermountain Healthcare, having had quite limited working contact with the North American scene, but have read and heard accounts of its focus on quality of care. Stan and I met only a few times, in the context of his Clinical Information Modelling Initiative (CIMI) and discussion about openEHR with one of his industry partners, fifteen years ago. In recent years, my stalwart GEHR and openEHR colleague, Thomas Beale, has developed close working and professional links with him.40 From what I gathered, it seemed that, in contrast with Jo’s situation, an opposite constraint impacted the generalization and dissemination of Stan’s work of those times, with industrial partnership in the work limiting options for open sharing of the methodology developed, within the wider health care world. This was not for lack of Stan’s personal efforts in the field. He worked hard to shape international agreement and alignment in the realm of standards for health record systems architecture, within the HL7 organization and the CIMI initiative, and in the realm of health care terminology, within the SNOMED organization.
Indeed, one thing that seemed largely to unite commercial interests through those decades was that open anything (especially openEHR, perhaps!) was seen as undesirable for health care record systems, except in support of a niche and non-competing, open-source medical records project focused on adoption in the developing world (openEMR). For year after year, from the time that I was running the website for openEHR from UCL, by far the greatest flow of traffic to the site came from the USA, and this correlated with a parallel and almost complete lack of USA-centred interest in engagement with its open and public domain-focused core mission. This was understandable and justifiable as home patch, market-protecting commercial strategy, of course. It did not bode well, though, for the creation and sustaining of more clinically focused, citizen-centred, mutually coherent, affordable and continuously evolving information systems that became increasingly necessary in support of high-quality health care more generally.
Unfortunately, and almost by default, commercial considerations of products, more than health care requirements, have tended to dominate the airwaves of this complex domain. And much time and money have been expended on avowedly collaborative international efforts that get bogged down when contrary national and commercial interests are in play, as they usually are. At the current stage of its evolution, a critical need is for a more inclusive, credible and trusted leadership and governance of the domain, which stems from, anchors and connects the coalface of health care, locally, with government health care and industrial policy and markets for health care IT products, globally. Health care professionals and care provider organizations need to advance their competencies and step up their contributions to this end. Failure in this regard has been a significant factor in the anarchic scene that has emerged in and pervaded health care of the Information Age.
In this quest, it remains a work in progress to discover how best to reconcile currently constrained business models for proprietary products and services in the health care IT marketplace, with governance and funding of collaborative endeavours that seek to create and sustain an evolving and dependable common ground of open specifications, clinical data models, software platforms and tooling, education and training, to enable a trusted and citizen-centred care information utility. Moreover, a shared resource that anyone, in any country and in any native language, is enabled and free to build on in the context of their personal, organizational or commercial health care related needs and ambitions. My collaborations with Jo Milan and Sam Heard were instrumental for me in creating and travelling the foundational years of such an endeavour, in the iterative and incremental creation and development of the vendor- and technology-neutral specifications, clinical models and tooling of openEHR and their international community interest governance. This I envisioned as a necessary enablement of a future information utility for health care, that could grow and prosper, as a global public good.
None of this is achievable by talking, writing and voting. It is achieved by implementing and learning thereby how to implement. openEHR has been an experiment exploring what could be achieved in a comparatively inexpensive and community-driven endeavour directed along these lines, deriving energy and motivation focused on enabling bottom-up ‘coopetition’ (eliding cooperation and competition). To have any chance of succeeding, it needed to discover ways to embed a culture and mission to collaborate and share methodology, to help the world of health care achieve and sustain greater value from the resources it does spend on IT, in meeting health care need. And to do so more flexibly and faster. Unsurprisingly, holding together the teams, environments and staying power required to remain steadfast in this ambition and to make progress, has, many times, been touch and go, over three decades! This a theme that I reflect on and take further in Chapter Eight and a Half and Chapter Nine. From the early decades, none of this would have happened without Sam Heard, who I profile next.
Sam Heard–East London Primary Care and the ParaDoc Practice Management Software
Fig. 8.12 Sam Heard–East London GP and co-founder of openEHR at Bart’s, UCL and Ocean Informatics. Now medical director for Aboriginal community health care services in Alice Springs, Australia. CC BY-NC.
Sam and I first met in the early 1980s when he was working as a GP in a newly established practice in Hackney within London’s East End. I was in the early years of my academic career in the Department of Medicine of St Bartholomew’s Medical College, a principal East London Medical School.
Hackney in those early days was a poor relation of the hugely affluent City Square Mile, situated close by. Its health care services faced many challenges that required bold and imaginative advocacy, resilient and charismatic leadership, and selfless devotion of its champions to the community they served. It attracted highly motivated doctors such as Sam, who built their practice there in the face of sometimes dismissive attitudes towards primary care among the powerful local establishments of secondary and tertiary care. These pioneers required strength of character and staying power of a high order. Sam was always upbeat and determined and became highly respected and loved among his peers and within the wider community. He participated fully in the medical education curriculum of the Medical College and in the professional training of GPs. His career demonstrates a very admirable pattern of devotion to the needs of depressed and deprived communities, which extends from these early days to his leadership today in the Aboriginal community health services in Australia.
The first example, that I observed first-hand, was when he taught himself the rudiments of a database technology of the era, called Paradox, and single-handedly wrote the prototype of a practice management and patient record keeping system for primary care. Drawing from his clinical experience and insight, this stood out for its focus on the clinical requirements and time constraints of everyday practice. He implemented the software within his own practice and demonstrated it to colleagues further afield, thereby persuading a consortium of East End general practitioners, among them our subsequent long-term colleague Dipak Kalra, to join in and fund professional programmers to continue the development and provide operational support services over the coming ten years. The ParaDoc system, as it was first named, and the associated GP consortium, became a national, rigorously accredited software product and provider. This substantial accomplishment owed its success to Sam’s innovative capability, drive and leadership. Dipak later took on this mantle and pursued with his mastery of administrative procedure, alongside Paul Julian, the senior partner in another East End practice, who was also closely connected with the Bart’s academic department. All the while, these people were full-time GPs working in a demanding clinical setting and fulfilling wider professional roles. It was a major voluntary contribution that stood out in its ambitious scope and challenging context.
The achievement evidenced in this example led on to and brought impetus to the development and subsequent worldwide dissemination of the openEHR methodology for standardizing electronic health records, as described in Chapter Eight and a Half. Sam has contributed massively to the openEHR mission, demonstrating exceptional commitment, and staying power. He has been a steadfast leader and colleague throughout testing times, sensitive to the values and needs of the openEHR Foundation and contributing much time and expertise.
I have known many key innovators in health informatics throughout the world during my career from the late 1960s. Staying power is a quality that has marked out the most successful among them, whose contributions have endured and grown. Recognizing Sam by conferment of the Order of Australia for the distinctive and distinguished, both practical and professional contributions he has made, was a powerful expression also of the importance of outstanding staying power, against often very formidable odds. Achieving and sustaining progress on such difficult challenges requires engagement at the centre of innovation and change, socially, scientifically and technically. Important causes Sam has served have not carried immediate prestige and have often been contentious. Progress has depended very considerably on the power of his insight and example.
Bill Aylward–Moorfields Eye Hospital and the OpenEyes Care Record

Fig. 8.13 Bill Aylward–ophthalmic surgeon, formerly Medical Director at Moorfields Eye Hospital in London, and founder of OpenEyes. Now an ocean sailor navigating the world with his wife in their catamaran, Double Vision, and pictured here on Antigua (2023).
Bill Aylward had a stellar career as an eye surgeon at the prestigious Moorfields Eye Hospital in London, linked with the Institute of Ophthalmology at UCL. He became its Medical Director and, on completing that term of office, devoted his considerable talents to sorting out the problems he had encountered first-hand, professionally and managerially, with digital eye care records. This led to the OpenEyes initiative, and our paths crossed in the first phase of the endeavour, as he assembled a team around him and launched into the work, on all fronts. He asked me to join his OpenEyes project board and he became a board member of the openEHR Foundation.41
The context in which we got to know one another was one of great change at UCL and its associated NHS Trusts. The UCL Institute of Ophthalmology, closely linked with Moorfields, is a key part of the UCL Biomedicine academic mission and a global leader in research. Each of UCL’s specialist biomedical research institute or hospital-based campuses has an important, close relationship with clinical services in its connected NHS Trust. UCL Biomedicine links with Great Ormond Street Children’s Hospital, Moorfields Eye Hospital, The National Institute of Neurological Disorders and Strokes, The Eastman Dental Hospital and The National Orthopaedic Hospital, as well as the Royal Free Hospital, UCL Hospitals and Whittington Hospital campuses.
In my time working as a head of department at UCL, from the mid-1990s, biomedicine activities had increased to constitute about fifty percent of UCL’s one billion pound per annum financial turnover. In those times, many UCL academic research institutes and departments, situated widely across north central London, ran independent IT systems and services, supporting their local activities. They wished to retain local autonomy in managing these, and to be funded for operating them, while still, and increasingly, drawing on and acting as rightful customers of the university’s central services, of course! And when Bill and I first met, around 2005, I had been given the role of leading an important aspect of institutional change, in persuading, encouraging and pulling together these separate teams into a coherent and integrated group and service, destined in time to become a large part of the central UCL-wide Information Services division. With each component team’s strong historic and everyday working ties to their local academic communities and related clinical service organizations, this was quite an ask in terms of harmonious and trusted change management! I draw on this experience in Chapter Nine, as an example of the creation of a new environment–a key challenge facing plans for realization of the care information utility.
There were, throughout, two further continuing tensions in play–between non-clinical and clinical departments of the university, and between the university and health care organizations with which the academic medical education and research missions closely connected. The latter extended nationally throughout relationships between the university sector and the NHS, covering wide-ranging technical issues of interface and compatibility of information systems, notably for maintaining security and confidentiality of personal data, while enabling clinically based teams to work efficiently in both their academic and clinical service roles and activities. This highly fragmented environment was a fertile ground for IT-related impasse and error! Helping to chart a trusted and achievable path forward was a wicked problem territory!42
But a tremendous bonus from this work was the opportunity it offered to me for building supportive alliances across the many parts of UCL and its related NHS Trusts that were touched by these issues. In anarchic times of transition, such alliances, and the trust and mutual dependencies developed through them, are invaluable. Many may feel safer in keeping their heads down and creating and living in a protected, siloed domain and environment. The nature of my academic mission precluded that as an option. I could achieve nothing of value if not seeking always to build alliances, to help me connect across such boundaries and barriers.
One such hugely creative alliance was with Bill, who was the driving force and innovator of OpenEyes. His reputation brought resources to his side and the Moorfields institution had capacity and was persuaded to invest. The software has evolved into a leading open-source medical record, now in use in approaching fifty percent of eye consultations across the UK, including at the heart of the national ophthalmology services for Wales and Scotland. Bill was hands-on in the design and prototyping of the software application, in the team and project management at Moorfields and in wider professional advocacy and fundraising from national and international organizations populating the world of ophthalmology. We co-supervised the work of a PhD student, Seref Arikan, who used the Moorfields clinical record repository as a testing ground for his research project, in which he built a formal framework of decision support and Bayesian predictive analysis on top of the openEHR specifications.
Bill had a talent for rapid engagement in partnerships and rapid decision and disengagement, as needed, when difficulties arose. The personality of a surgeon, you might say–he was an exceptionally capable one. He engaged in racing dinghies as a hobby and cooking cordon-bleu quality food, in everyday life. The range of clinical and organizational partnerships he drew together in the cause of OpenEyes, including the Royal College of Ophthalmology in London and international charities, such as Orbis, was astonishing.
The development team Bill created drew strength from him, but the going was tough, and it was his sparkling talents and capabilities that held things together and drove the project forward and into use. It was early prototype software, and institutions hosting prototypes have a tough time, too. In the subsequent years, OpenEyes consolidated into a commercially viable mission, but the first ten operational sites are usually as demanding and difficult to establish as the following one hundred, following my interpretation of the Penrose law of squares that I describe in Chapter Nine.
In his roles as clinician and Medical Director, Bill had experienced the difficulty of providing and sustaining clinically focused and useful software for use at the coalface of care services. He had seen the progressive disconnection between software systems and the evolving functional and operational requirements for their close integration with clinical practice, leading to the problems that accumulate in efforts to sustain such systems, as requirements and technologies evolve. OpenEyes was born of his close observation and engagement with the difficulties he had faced with the then current electronic records system at Moorfields. This had grown, topsy-like, as a proprietary commercial software, gradually leading to a tangled web of data relationships, confounding the clinical management of patients and operational management of the institution.
Bill saw national clinical community involvement in oversight of the design and development of OpenEyes as of paramount importance. To encourage this wide professional engagement, his vision was of a clinically focused and led open-source care record to support practice at the coalface of care. It was to be tuned to the needs of both clinicians and health care organizations and their IT support services. Bill brought to this mission all his many talents as a highly intelligent, practically accomplished, energetic and streetwise soul. He understood and knew from training and experience what and how the clinician needed to capture and use entries in the care record, throughout the life cycle of the presenting eye condition and its treatment. Combined with his polymath skills, this gave him special insight and capacity to innovate. Like Tony Shannon at Leeds, who worked with my team at UCL on the first stages of creating an open-source openEHR platform, as described in Chapter Eight and a Half, he was a strong advocate of open-source software and clinical community-led governance of its design. He was publicly very critical of the NHS National Programme for IT (NPfIT). He used to take an NPfIT labelled coffee mug to brandish at his talks, saying it was just about the only thing the programme had given him, as a practising clinician! Others might say they had also been given a lot of headaches!
The OpenEyes software was envisioned and brought to life from the inside of the wider ophthalmology clinical community that Bill engaged. Like John Dickinson, Octo Barnett and Sam Heard, Bill saw no impediment or reason not to write his own code, to explore and enact his vision of what he and the wider community needed, in realizing his dream. As I saw with Octo’s, John’s and Sam’s code, there were deficiencies and vulnerabilities that needed to be ironed out in making their ideas and products long-term coherent, performant and sustainable, but their unique insights and capabilities to work across disciplines was what made them and their contributions special and significant. Bill devised and implemented a program that enables clinicians to record efficiently the problems encountered in clinic sessions. It embodied a flexible interface through which essential features were recorded on a graphical template diagram. This was the EyeDraw software that he developed, which was contributed to and used to great effect by his PhD student, Maria Cross, working on the depiction of family trees.
As time went by and step by step, the requirements of the multiple ophthalmology sub-specialties were attended to, adding further modules to the OpenEyes software. The team devised the means to integrate this record with the specialized instruments used in assessing and measuring eye performance and health–such as intraocular pressure and visual acuity measurement, visual field defect mapping and other imaging methods. They understood how data needed to be aggregated and integrated with other computer systems, within and between departments and institutions, and the standardization of method and recording needed for these data to be reliably accurate. A growing group of clinicians and adopting NHS Trust IT service leaders met as a board, to advise on requirements and design. These early adopter NHS Trusts provided significant development funds and their commissioned software companies provided software development and installation support. The resulting, increasingly performant and impressive OpenEyes product was introduced to professional meetings and succeeded in tenders for new installations around the country.
Alongside Bill, from the start, was another formidable clinical and polymath talent–James Morgan, Professor of Ophthalmology, and general all-rounder star at Cardiff, who later took on the project leadership role, as Bill withdrew. Also close by was Peng Khaw, the luminary pioneer of glaucoma care at Moorfields. With Peter Coates at the Apperta Foundation, David Haider from Bolton, and Andy Barker from East Kent–the latter two having been early adopting Trusts in the NHS–the ongoing updating and development of the software settled into a gradually more sustainable product ecosystem, working with software development partners, Jason Brown and Clayton Blake of the ABEHR and ToukanLabs companies. Carole Jones and Michelle Teo later joined the Board–Michelle still a trainee ophthalmologist but with the distinction of having already won a Google entrepreneurship competition.
The OpenEyes project went through several phases of evolution–detaching from some people that Bill had employed, who proved ill-equipped to consolidate the progress, and from the Moorfields Trust management that was going through its own difficulties and felt unable to continue support. The mission was helped in this transition to a new structure, independent of Moorfields, by my colleague and friend Sarah Hamilton-Fairley, who I had worked with for many years on her StartHere Project. I return to this connection in Chapter Nine. There was some debate about the software IP relationships with Moorfields and potential business models for expanding the project, internationally. Bill’s focus was always towards making OpenEyes an international exemplar of doing better, as an open-source initiative. This was organized first, in-house, at Moorfields, then as an independent charity owning the OpenEyes IP, and finally under the aegis of the Apperta Foundation. Through these stages, we experimented with different ideas for consolidating and sustaining the mission, and then extending it, through fledgling commercial partnerships. It has been a long runway, but the project has taken wing, and is climbing–the crucial importance of grounded mission and staying power, once again fully in evidence.
Bruised by the internal strife at Moorfields, which consumed time and energy and wasted much money, Bill’s long-ago expressed ocean sailing ambition reasserted itself, and he and his wife started to prepare. At this vulnerable moment in time, project leadership of OpenEyes passed to James Morgan, with his ‘can do and does’ character, like that of Bill. He and David Haider held together the, by then, some twenty-strong, clinical advisory group. And as adoption further widened, the entrepreneurial elan of Peter Coates at the Apperta Foundation and the company partners helped to consolidate and chart an increasingly confident dissemination pathway for the product, to the point where OpenEyes is regularly winning tenders for NHS hospital and community systems. As mentioned above, it is now the national platform for eye care records in Scotland and Wales and adopted in some ten large NHS Trusts in England, combining to provide the records for fifty percent of national eye care consultations. OpenEyes has been an amazing story of survival through thick and thin, to become the software it is today. It is easily and quickly spun up as a tool, on Cloud platforms across the world, and a trail blazer of new approaches to care information utility, as I discuss in Chapter Eight and a Half.
Thanks to its outstanding pioneers and their clinical vision and staying power, the OpenEyes initiative has proved its metal in delivering high-quality software that provides value for money. Its goals are humble and humane, dependent on its strong and wholehearted, clinically active leadership, pitched beyond the commercial and industry-led focus that has characterized much of the big tech era in health care IT.
My personal focus within OpenEyes, apart from as a founding management board member and trustee, is in exploring its usefulness in support of busy and overburdened services in developing countries, and in helping meet wider needs of patients throughout their history of eye-care. We see a viable pathway opening for it to become a global utility, safely and sustainably. As young and developing eyes are increasingly focused on mobile phone and other close-by screens, a pattern of increased prevalence of early eye problems is being seen.43
Bernadette Modell–UCL and the WHO Collaborating Centre for the Community Control of Hereditary Diseases

Fig. 8.14 Bernadette Modell–epidemiologist at UCL and Director of the WHO Collaborating Centre for the Community Control of Hereditary Diseases. CC BY-NC.
One day, out of the blue, the genetic epidemiologist Bernadette Modell, a world authority on the genetics of hereditary diseases, came to visit me. She worked in collaboration with a clinical team in the Haematology Department at the Whittington, led by Beatrix Wonke, which provided leading care for the many thalassaemia patients living in the local community. She came to discuss her interest in creating information systems accessible to the affected communities she worked with, and to explore potential for collaboration with my department, CHIME.
North Central London is home to ethnic communities that originate from countries where genetic variants of the haemoglobin protein are prevalent. These variants are associated with abnormal structure of the red blood cells that distribute oxygen and carbon dioxide around the body, in respiratory gas exchange. One such disorder is thalassaemia, a complex and life-threatening disease requiring regular mitigating clinical interventions and lifelong care. The disease is endemic in countries where malaria, transmitted by mosquitos, is an everyday threat. The haemoglobin gene variant has persisted, it is suggested, because it provides some protective advantage to the population, in resisting malaria.
The mathematics of the affinity of the haemoglobin molecule to capture oxygen and carbon dioxide within its structure, in different prevailing acid-base balance conditions of the blood circulating in the body, was something I knew well from my mathematical modelling days with John Dickinson. I had optimized models of this changing dynamic to analyse respiratory gas exchange in critically ill patients at Bart’s, as described in Chapter Four. In that situation, the haemoglobin molecule was typically in good shape, but the gas transport and exchange, through lungs, circulation of blood and tissues, was under abnormal stress.
One of Bernadette’s principal goals, which I felt fitted well with CHIME’s wider mission, was to focus national and international attention on creating an information system supportive of consistent and contextually appropriate advice for the thalassaemia patients and their families. This had echoes for me from my time years before, working with Bob Jones, Ilora Finlay and the Marie Curie Foundation, developing a videodisc-based educational resource to support multiprofessional care for cancer patients and their families at home. It was that connection that had led me to my involvement in the project creating a tropical medicine education resource for the Wellcome Trust.
Bernadette brought the World Health Organization (WHO) Collaborating Centre for the Community Control of Hereditary Diseases, of which she was the Director, into CHIME, to align with the informatics interests of our Centre. She became a much-valued, inspiring and supportive colleague of those times. She was a wonderful supervisor of research students and her international network of collaborators brought connection with inspiring leaders like Arnold Christianson in South Africa, adding lustrous global context to our local academic community.
Bernadette and I co-supervised Matthew Darlison in his PhD project to design and create the APoGI (Accessible Publishing of Genetic Information) resource. In this, Matthew formed close personal links with both the local thalassaemia clinical team and their patients. It was a difficult endeavour, both in its design and implementation, because of the complexity inherent in the manner of its expression, relevant to the needs of individual patients and others seeking guidance. A further context was that of population screening for the disorder, and counselling services communicating about the risk of its transmission to following generations. The lead clinician for the national thalassaemia services in Iran, also became a PhD student of Bernadette in CHIME, visiting as often as she was able.
Through Bernadette, the care environment that I discovered and was privileged to be welcomed into and become involved with was exemplary in many respects relevant to this book. It connected global scope of the clinical problem addressed, with how it was coped with and tackled locally. It embodied clarity of purpose and goal, centred on listening to members of the affected local community and learning about its needs–what mattered to them–and helping and supporting them. It had a balance of motivation, mutual support and dynamism on all sides–the patients and their community, the NHS clinical community and the academic epidemiology community. There was powerful motivation for these groups to work together to tackle the multi-faceted challenges they faced, and this showed in their mutual trust and respect. It was a holistic environment and there was supportive synergy in all their efforts.
The clinical disorder and dysfunction of haemoglobin is deeply consequential for the everyday lives of affected patients and their families in the community. The clinical science and practice that strives for improved treatment connects with a rigorous timetable of hospital visits, and stays. The genetic epidemiology connects local understanding and communication about the disease and its consequences, with experience of the impact of the disease on the provision of services in other countries and cultures. Each group would have been much less effective in achieving its goals, had they not been drawn together and worked collaboratively in this way.
Bernadette’s work in the WHO Centre was impactful in raising awareness of the global burden of non-communicable diseases. In terms of wider advocacy for the work, we succeeded in interesting the City of London Livery Company for the IT industry, in running a national walk to raise money for its support. We also tried, but failed, to engage national policy support for the APoGI approach to providing context-sensitive information for patients in national screening programmes for genetic disorders. Funding of its further development was difficult to secure as it was seen to fall awkwardly between the two stools of research and practice. Policy makers were attuned to top-down more than bottom-up perspectives of how screening programmes should operate, and there was a melee of such ambitions in play. Bernadette and Matthew were focused on creating information utility tuned to local community needs and synergy with local clinical practice, building outwards from this in wider advocacy and community engagement, both nationally and internationally. The need to ground such services in local knowledge accords with the reality that the needs for preventative care are typically found to be greater within poorer and more deprived communities, where personal options are more limited, and that such communities, as in North London, sit cheek by jowl, locally, in a chequered landscape, alongside much more affluent ones.
National service development initiatives, each jostling for attention and funding, came and went with great rapidity in those years. The resulting regularly disrupted pattern had the effect of blocking rather than enabling sustained innovation in services, which require a long-term focus, well beyond the few years of each electoral cycle. This too rapid turnover of initiatives risks poorly configured services beset by noise and bias of data.
Trends Shaping Future Care Information Utility
The purpose in creating a coherent and connected care information utility is not to cure the problems of the past, but to learn from them in helping to shape and create a better future. It is not about reforming health care; rather it is about helping to reformulate and reinvent it to serve the future Information Society. The pioneers I have highlighted in the preceding section are some of many I have encountered and learned from along my songline. Each in their own way has responded to that need in their commitments and actions. It is, of course, an ever-changing mission, as the Information Age moves on. The story now switches from microscope looking back to telescope looking forward to what may lie there. There is no Hubble or James Webb telescope equivalent able to help us probe back in time, to illuminate our understanding of where we are now, and project forward to what the future may hold. We must invent and create our imagined and desired future of health care.
The WHO has defined health as ‘[…] a state of complete physical, mental, and social wellbeing and not merely the absence of disease or infirmity’.44 It is clearly the case that information technology has led to astonishing and transformative new scientific insight and capability to combat disease, resulting in both greater lifespan and correspondingly greater proportion of chronic disease and disability. It is clearly not the case that society of Globalton yet enjoys a state of ‘complete’ wellbeing; life there for many is more challenged, anxious and uncertain than was Localton life.
Human actions, as well as natural disasters, perturb both local and global ecosystems and communities, with consequent adaptations over indeterminate time. Short-term gain can turn to long-term pain. Long-term action can be required to rectify short-term inaction. Health care interventions that may appear attractive and strengthening, in the short term, may lead to longer-term harm–the over-prescribing of antibiotics comes to mind. Human resilience is hard won and easily lost. The milieu intérieur of Claude Bernard (1813–78) is hard-won bodily defence–that defence, evolved and tested over millennia, may be weakened, and overwhelmed, over millennia, too. Medicine has rightly been a conservative profession. As we promote conservation of environment, so we must promote conservation of health. Information utility must serve that end.
The two inverted triangles of Richard Smith’s editorial characterize the era of Whitehead transition of health care services, from what is described as Industrial Age medicine to Information Age medicine (see Figure 7.10). They focus on the relative volumes and costs of services, from costlier, low-volume acute hospital care to cheaper and more extensive home and community-based care and self-care. The horizontal width at each vertical level of the triangles represents volume of services provided at that level, and the side bars indicate relative focus and cost. They do not attempt to reflect utility–value that derives from the efficiency and effectiveness of services. Let us think of the lower triangle as also representing my Localton experience, in terms of the reality of how things were then in village life. As I recounted in Chapter Seven, mutual care and self-reliance were, of necessity, more the order of the day.
Information technology deployed in this era of transition has been focused in broadly three directions: improvement in methods powered by advances in science and engineering, to achieve greater insight and effective intervention (imaging, genomics, pharmaceutics, machine intelligence, robotics); improvement in service delivery, powered by new possibilities for both specialist and self- and community-based care, surveillance, prevention and early intervention; improvement in governance, driven by changing population-based data, ethical and legal concerns and social and cultural change.
Suppose we think now about IT investment within the two triangles and how it encourages and facilitates the transition from the top to the bottom triangle. The greater investment focus, by far, has been into the costly hospital care settings of the top triangle. The lesser by far into community and self-care settings of the bottom triangle. The new money in the Information Age has followed the old money, into further support of Industrial Age medicine and at the expense of enabling and supporting Information Age health care to come of age. Investments come from different sources and push in different directions, and thus in some cases cancel one another–investments sum as scalars, directions of travel sum as vectors. Costs add up, progress is a Brownian movement.
The UK Poet Laureate Simon Armitage wrote a beautiful poem for the 2020 National Poetry Day (4 October).45 It gives an optimistic vision from his own village in the North Country, of Globalton experience in the Covid crisis. It is an evocation of how global village life might be experienced, from beyond the transition to the Information Society. An optimistic vision of connectedness and cohesion, stretching and empowering human potential and challenging the individual citizen to take charge and not fall victim to dystopian vision of disconnectedness and fragmentation. In health care, this sense of personal control and self-reliance is not widely experienced today. How can the culture of self-reliance, mutual support and cooperation, essential in Localton life, translate to Globalton life, which interacts and impinges globally as well as locally?
For health care services that support the WHO vision, balance and continuity of a coherent and comprehensive information utility must be a clear and trusted goal of the bottom triangle. It must as well be an enabler of the transition from top to bottom, centred on care of the individual citizen rather than, as now, on the management of services. The design and development of such a utility must respect and reflect the citizen’s capacity to understand, learn and grow, and their need to know about and be involved in their care. Citizens, for their part, must understand and acknowledge that there will often only be good and bad, better and worse, ways of acting, not right and wrong ways, and they are party to their enactment, for others as well as for themselves. This balance will require local governance and community leadership, exercised from below rather than by fiat from above, in the Taoist tradition of leadership. Such a utility, supportive of lifespan and lifestyle, consonant with economy and environment, realizable with capable and trusted professional services, leadership and governance, will be a considerable test of human ingenuity, commitment and staying power.
This qualitatively different, citizen and professionally focused care information utility, can only be centred on data and record that integrates and connects health and care. There will be many evolutionary changes and adjustments required in the framing and sharing of knowledge and discipline, in professional practice and in education and governance. The information revolution and its impact on health care, as discipline and as practice, has presented everyone involved with a great deal of change, to be coped with and adapted to. It has surfaced and highlighted issues of understanding, choices and values, which go to the heart of how services reason, decide, act and record what they make and do. It has imprinted Internet time onto these changes, that need more time for learning how. It has comprised a giant black swan era–lasting fifty years, but black swan, nonetheless. Realistically, we are only halfway through this anarchic transitional era and its challenges for coping, as we all do our bit to shape and create a very different world. It is a vulnerable and manipulable era.
Knowledge and Discipline
Discipline is an assertion of rules of knowledge, belief, and behaviour. It operates to keep order within the boundaries of a defined domain, and defend against usurper and interloper, coming from outside.
This is implicit in the term. I can still recall my feisty first Latin teacher starting each class with salve discipulos [Hello, (or Be well) pupils], said loudly, to wake us up! And we pupils noisily responded, salve magister [Hello, teacher]! I cannot imagine that anywhere in the school culture of Globalton, today! Discipline connects pupil and teacher, citizen and sage. And academic discipline has changed at an incredible pace in the Information Age and continues to do so, connecting many domains of knowledge. Whitehead made an observation about scholarly caution in the face of this trend, that still resonates today:
Your thoroughgoing scholar resents the airy speculation which connects his own patch of knowledge with that of his neighbour. He finds his fundamental concepts interpreted, twisted, modified. He has ceased to be king of his own castle, by reasons of uncomfortable generality, violating the very grammar of his thoughts.46
The culture and practice of medicine has strong foundations in craft, apprenticeship and accepted procedure. Professional skills, honed over a lifetime of practice, are not always easily formalized within boundaries of discipline. A radiologist looks at thousands of images, over time, and learns how to interpret them in their clinical practice and context. A GP draws on the experience of observing and listening to the narrative of many patients’ lives, when discerning the clinical issues in play for a particular patient, at a particular time and place, and how best they may be approached and understood.
Imbalance and disconnection of knowledge and experience are weaknesses easily amplified in the Information Age, through bias, corruption and overload of information. These dangers were anticipated in different ways by Albert Einstein (1879–1955) and Whitehead:
All knowledge of reality starts from experience and ends in it.47
The consequences of a plethora of half-digested theoretical knowledge are deplorable.48
One remedy for disconnection lies in focus on reconnection, revisiting boundaries of discipline and profession and connecting their sources of knowledge and experience. Information as we have seen connects knowledge and action. It also connects knowledge with experience.
Some twenty years ago, I worked on summarizing the interdisciplinary connections of health informatics across UCL. This was initiated by the then UCL Vice-Provost for Research, my medical physics colleague of years before, Dave Delpy, who went on to become Fellow of the Royal Society and Chief Executive of the Engineering and Physical Sciences Research Council of the UK, and Anne Warner (1940–2012), a biologist and head of an interdisciplinary centre established at UCL to foster connection between the mathematical, physical sciences and life science and experimental medicine, arranged to give the name CoMPLX. These are two diagrams we constructed to capture the issues (Figures 8.15 and 8.16).
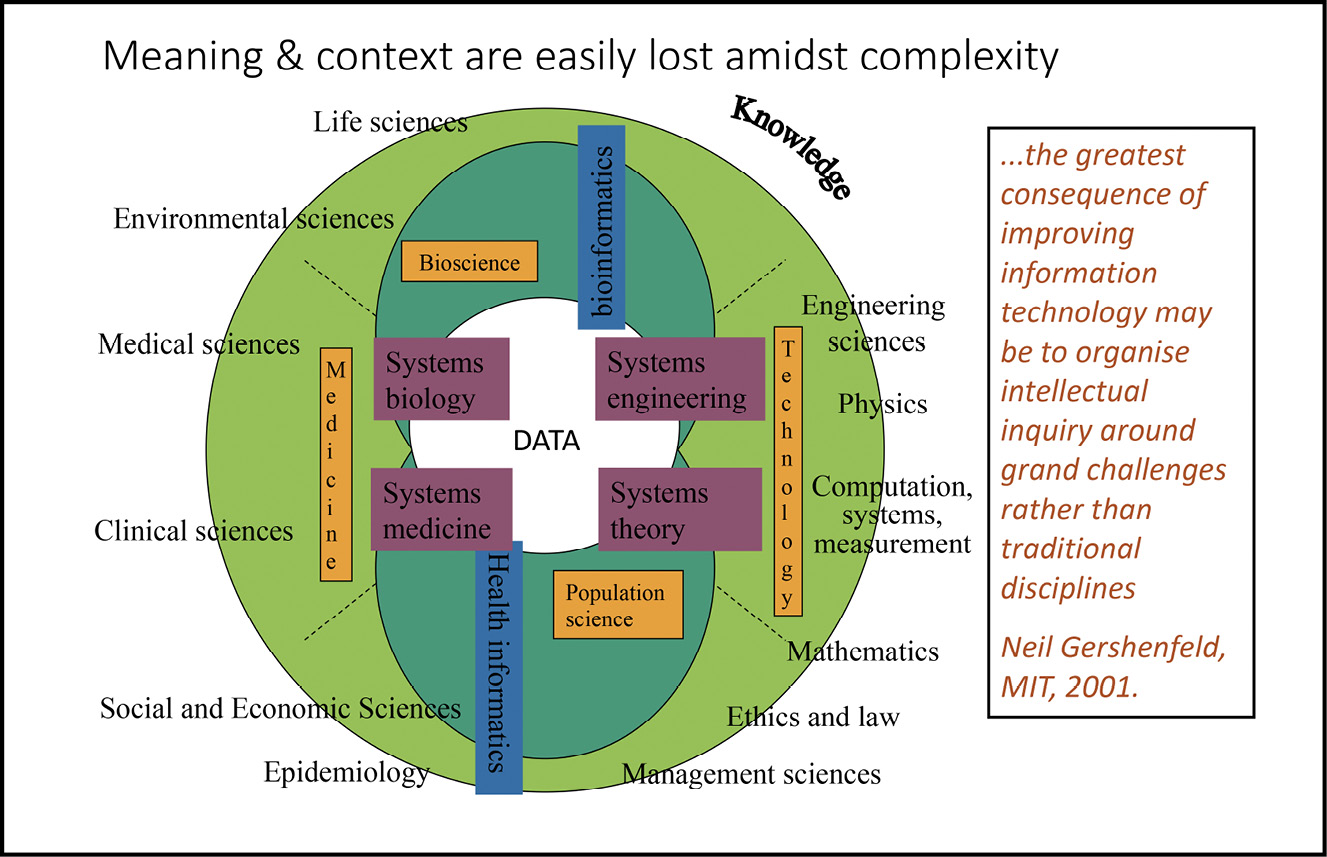
Fig. 8.15 The interdisciplinary science of medicine, connected around Ranganathan’s circle of knowledge. Image created by David Ingram (2010), CC BY-NC.

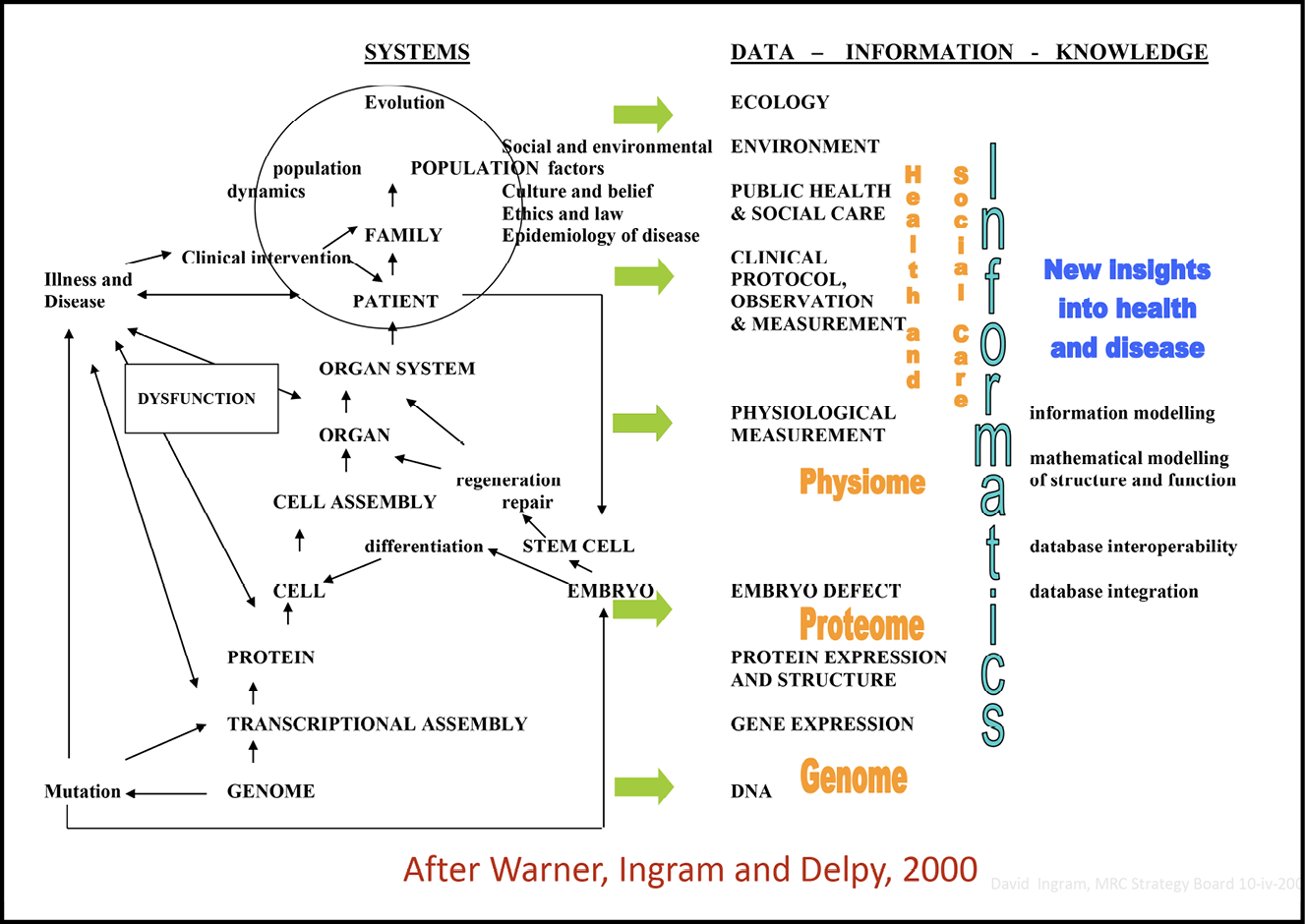
Fig. 8.16 The connected information landscape of human biology and medicine. Image created by David Ingram, Anne Warner and Dave Delpy (2000), CC BY-NC
.
The focus and governance of interdisciplinary science was the subject of much debate and prediction, suggesting growing connections grouped around what were called ‘grand challenges’, as explored by Neil Gershenfeld, at Massachusetts Institute of Technology (MIT).
The greatest consequence of improving information technology may be to organize intellectual inquiry around grand challenges rather than traditional disciplines. If this turns out to be so, then a title like the physics of information technology may eventually become triply redundant the truth is that none of those words can properly understand without all of them.49
This approach was being championed by the Provost of UCL, Derek Roberts, at the time I re-joined the University in 1995. He came to meetings that he organized to encourage partnerships among disciplines, equipped only with his formidable personality and a single overhead slide, depicting an unlabelled set of overlapping ellipses. This he used as his sole visual aid, ascribing the ellipses to different departments, and faculties, as he spoke, according to the occasion! His aim was to encourage innovations stemming from common endeavour shared across disciplines. He wanted these to become vectors of advance, coordinated within and across existing disciplines, not as supplementary and separate islands of new discipline.
In the following years at UCL, this became a continuing goal of Vice-Provosts for Research. After Dave Delpy, David Price proposed a wide-ranging set of interdisciplinary grand challenges, chosen to bring together disciplines from all around the Ranganathan circle of knowledge (see Figure 2.2). These were global health, sustainable cities, cultural understanding, human wellbeing, justice and equality and transformative technology. They echoed the saying of Einstein that ‘All religions, arts and sciences are branches of the same tree’.50
As I have already mentioned, in a footnote above and in Chapter Seven, a complementary practical challenge for the university involved designing and implementing corporate research computing facilities and associated training courses, and integrating many and diverse existing IT support teams, whose loyalties were to the department in which they were situated. It was an exercise in finding common ground and creating an environment supportive of the dual goals of local and global community. It was a challenge of maintaining the local environment that was an important and valued home for its staff, while engaging everyone in creating a strategy for transition towards alignment within an evolving and standardized, university-wide framework of information services. It was a human challenge of helping people put aside their fears and anxieties and step safely from one comfort zone to create a new one, working together in maintaining geographical ties to their local communities while evolving new working relationships more widely.
The same issues existed in the context of local NHS Trusts and the connection of academic research and education between the NHS and the university. This is a slide I used, highlighting the different perspectives in play, in building these bridges:
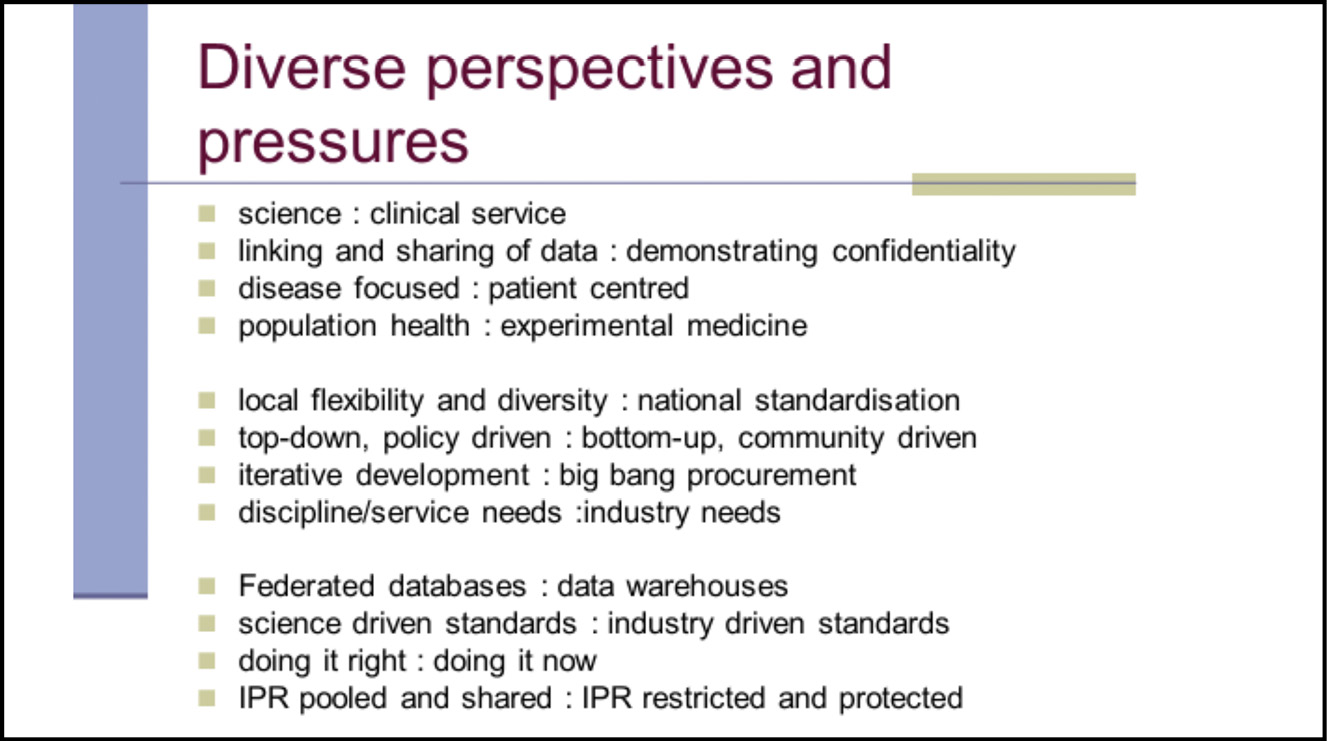
Fig. 8.17 Diverse perspectives in play when seeking to bridge academic, clinical service and industry domains of health care information. Image created by David Ingram (2010), CC BY-NC.
The central role of information infrastructure in enhancing research capability and capacity is illustrated in this morning’s (7 October) announcement of the award of the Physics 2020 Nobel Prize to Roger Penrose, Reinhard Genzel and Andrea Ghez.51 This synergistic interrelationship is as true, now, in the life sciences. And improved information utility is a prerequisite of health care services becoming part of a virtuous circle of progress and improvement in health care, enabled by advances in biomedical science and engineering.
Research priorities have driven academic investment in the research computing services that have powered transition into the Information Age, creating and benefiting from shared computational methods and resources, implemented and operated through funded collaborations between universities and industries, internationally. Where requirements are specific to one discipline or group of disciplines, that community creates its own bespoke services. Astronomy, physics, bioinformatics, natural environment, social science–all created specialized national centres. Clinical research was a special case, where individual projects and programmes had requirements for gathering and integrating data from outside the academic domain, from health care institutions that do not share common basic infrastructure, and where operational data were substantially incompatible, from one institution to another.
The Medical Research Council faced this issue with multiple long-term population studies, each with its own needs, each having created its own bespoke information systems. The multi-year European Union Advancing Clinico-Genomics Trials on Cancer project encountered similar difficulties in integrating diverse cancer treatment datasets. The situation became increasingly onerous, expensive and intractable. The Royal Marsden Hospital experience described above showed the clear benefit, to both local institution and global domain, of coherent data management. A 2022 report from the health IT industry body, HIMSS in the USA, charts the number of medical record systems of different companies that individual health providers are using.52 On average, each hospital is running sixteen different electronic health record platforms, and each vendor of hospital systems is connecting with eighty-two other vendors’ records, with no common information model to underpin their clinically meaningful interoperability.53 Coherence is of equal significance, and yet more complex to achieve, between institutions and across national boundaries. openEHR has pioneered openly specified and standardized clinical data modelling for care records, translated across languages, and an open platform for implementing them. This is steadily disseminating to provide common ground for institutions and sectors of health care, globally, as described in Chapter Eight and a Half.
As requirements to be met by standardized systems become more extensive and complex, connecting multiple domains of knowledge and discipline–for example, in health care, embodying phenotype, genotype, environmental and social science data–human capability and capacity issues assume ever greater significance. How will the nature of professions and educational needs change in the transition to the future Information Society? These are issues that connect with every citizen and are thus, inevitably, disruptive and contentious matters.
Professional Practice–How Information Technology Will Change It
How and why professional people specialize and practise their skills and trades is highly personal. Interest, challenge and satisfaction in work, wealth, prestige and power in position, all factor in. Assessment and regulation of professional practices centre on issues of trust–in knowledge, expertise, behaviour and ethics. How and why their clients need, trust and engage with them is also personal.
In thinking about this section, I have been reading, again, The Future of the Professions, by father and son, Richard and Daniel Susskind. It is a great book–comprehensive, detailed and reflective, but also pressing and passionate–a delightful mix of father and son. Richard is eminent in IT and law and Daniel in economics, with experience of work in central government policy circles. Together, they bring a wide range of ideas and examples. The book is authoritative and contains important commentary. It identifies implicit imbalances of knowledge between the professions and the public they serve, that synchronize them in a status quo of relationship and trust. It describes the trends in information and technology that challenge this status quo, pushing and pulling fundamental change.
They summarize what they call the Grand Bargain between professions and society:
In acknowledgement of and in return for their expertise, experience, and judgement, which they are expected to apply in delivering affordable, accessible, up-to-date, reassuring, and reliable services, and on the understanding that they will curate and update their knowledge and methods, train their members, set and enforce standards for the quality of their work, and that they will only admit appropriately qualified individuals into their ranks, and that they will always act honestly, in good faith, putting the interests of clients ahead of their own, we (society) place our trust in the professions in granting them exclusivity over a wide range of socially significant services and activities, by paying them a fair wage, by conferring upon them independence, autonomy, rights of self-determination, and by according them respect and status.54
They admit this is a trifle legalistic–as my paediatrician wife, a believer, would say–as she sometimes does, understandably, of wordy things written by the agnostic me–Amen!
Before confronting the challenges to their Grand Bargain in the Information Age, the Susskinds detour, as I have, frequently, in this book, into its history and context–George Bernard Shaw (1856–1950) and his description, in The Doctor’s Dilemma, of the professions as ‘conspiracies against the laity’; the happy hunting ground enjoyed by sociologists in exposing and unpicking the bargain; and its Marxist framing within the language of the struggle of capitalism and the proletariat.
The central focus of their book is embodied in its strapline: ‘how technology will transform the work of human experts’. They explore alternative ways of organizing professional work and consider to what extent human beings are indispensable in delivering this and whether professionals are to be trusted in making such judgements. All this within incisive questioning of the extent to which the Grand Bargain remains fit for purpose in the Information Age–is it serving society well?
The first of three broad sections surveys professionalism and change in health, education, divinity, law, journalism, management consulting, tax and audit and architecture. It surveys patterns of transformation in skills and competencies, configuration of work, workforce structure, customer choice and the preoccupations of professional firms as their trade becomes demystified in the Information Age. The second broad section surveys the onward march of information and technology and the production and distribution of knowledge. The third section looks forward to the implications of change in professionalism, in more human terms–trust, morality, empathy, personal identity with craft, work, trade and human interaction, and where these are leading, and choices to be made in shaping them. They are almost universally cautious of exclusivity (an enclosure of knowledge and knowhow) and prefer to focus on a decades-long evolution towards open commons as a means for democratization of knowledge.
They ask the question ‘To what problem is professional work the solution?’ They propose ‘access to knowledge’ as the ‘hole in the wall’ or need that professional work drills and fulfils.55 Knowledge and the imbalance in human knowledge are at the heart of professional work, and this imbalance underpins the Grand Bargain. It is a changing landscape in human social evolution, and as machines progressively take on aspects of professional work (for example, book-keeping substituted by accounting software) and become more ‘knowledge-full’, the balance and the power it confers, also change. In considering implications for professionalism in the Information Age, it is on this changing balance that they believe the focus should lie. The trust, reassurance, quality, status, training and regulation components of the Grand Bargain are, they suggest, secondary matters.56
In the context of health care services, access to knowledge has been transformed out of all recognition along my songline, for professionals and public alike. Knowledge has flowed over, washed away and tunnelled through and under barriers and boundaries between disciplines, professions and services, and those they serve. The nature and organization of the health care professions, the education and training programmes and assessments that aspiring entrants pass through, the regulatory frameworks that govern them along the way, all combine to shore up professional barriers under siege. Access to knowledge is a battering ram that knocks them down; like Venice, defended with flood barriers to ward off the inevitable. They create new points of contention and vulnerability that also come under siege, to allow the rising tide to flow through.
The Susskinds conclude with questions about what we should do, and first ask, what future should we want? In the context of health care, this echoes in my mind back to Douglas Black (1913–2002) and his BMJ leading article in 1982.57 Do not set out to computerize without thinking first about the requirement you are addressing. Their book discusses two broad paths ahead in the Information Age–more efficient ways of working based on what we do today, or gradual replacement of professional work by increasingly capable information systems–two paths in the Robert Frost wood. The path most travelled is the former. The AI fallacy they write of–as Richard Feynman (1918–88) did, more generally, long before–is that such systems will be based on how professionals create and distribute knowledge, today. They argue that:
In an era of increasingly capable systems, the professions, or elements of them, should survive and prosper because they bring value and benefits that no system or tool can; not because we regulate competitors out of the market, nor because we cannot imagine a world without the professionals, nor again out of nostalgic impulse for a fading way of life.58
Their view, captured in the book’s flyleaf, is that ‘In an Internet society, we will neither need nor want doctors, teachers, accountants, architects, the clergy, consultants, lawyers, and many others, to work as they did in the 20th century’. In conclusion, they place liberation of knowledge and enclosure of knowledge in counterpoint. They estimate human society will favour the former, and place their personal marker on this, saying finally, ‘We now have the means to share expertise much more widely across our world. We should also have the will’.59
The bifurcation of choices that the book highlights feels close to that which I focus on in Chapter Nine, in the search for common ground based on Open Society and Creative Commons. I came to this, though, after two decades in which I had focused on information technology for medical education. The future of education in the Information Age is as disruptive a prospect as that for the professions it prepares for. This is where the storyline now moves on to.
The activities I initiated and led at Bart’s from 1990–95, to create a joint medicine and nursing clinical skill teaching centre–combined with leadership of multidisciplinary, multiprofessional and multi-sector EU projects on health record architecture–brought our group to the notice of the leadership of UCL and the Whittington NHS Trust. As a result, I was invited in 1995 to establish the UCL Centre for Health Informatics and Multiprofessional Education, which I led for the next fifteen years up until my retirement. This placed us at the centre of the development of the newly merged UCL and Royal Free Medical Schools and Postgraduate Institutes. It positioned us to explore academic connections of health informatics with clinical education, research and practice. This was a local grand challenge, leaving aside the wider implicit pursuit of new academic community and discipline of health informatics in its connections with the wider health economy, nationally and internationally. This mission involved a great deal of trust and a great deal of challenge. In microcosm it connected with and embodied, in practical everyday terms, the wider dilemmas faced by health care in transition to the Information Society. I reflect on this environment, its successes and failures, the exhilarating freedoms, and unnerving challenges of creating and leading it, and its legacy, in Chapter Nine.
Education–Environment for Learning
The transition from Industrial Age to Information Age medicine, highlighted by Richard Smith’s two triangles (see Figure 7.10), is paralleled in education–learner focus mirrors patient focus, self-directed learning mirrors self-care. Roles, costs, performance and accountability of services and institutions, and equity of access to them, face increasing scrutiny and challenge in education, as they do in health care.
Questioning of the rationale of education services is not new, but information technology has fundamentally changed the playing field. Transformed access to knowledge, teaching and learning resources, and related assessment methods, have thrown new light on lifelong learning and the interface of education and practice, in formal study and apprenticeship. This has been accompanied by a changing perspective, and ‘radical uncertainty’, in Mervyn King’s phrase, about the permanence of work, ways of working and lifelong careers. The ways in which different educational institutions have adapted to the risks of Covid-19, to work in different ways and embrace a different mix of technology and access, have added contemporary impetus and opportunity for constructive change.
Whitehead was questioning the role of universities a hundred years ago.
The universities are schools of education, and schools of research. But the primary reason for their existence is not to be found either in the mere knowledge conveyed to the students or in the mere opportunities for research afforded to the members of the faculty. Both these functions could be performed at a cheaper rate, apart from these very expensive institutions. Books are cheap, and the system of apprenticeship is well understood. So far as the mere imparting of information is concerned, no university has had any justification for existence since the popularization of printing in the fifteenth century. Yet the chief impetus to the foundation of universities came after that date, and in more recent times has even increased. The justification for a university is that it preserves the connection between knowledge and the zest of life, by uniting the young and the old in the imaginative consideration of learning.60
Illich was questioning the nature of schooling, more widely, fifty years ago. As shown in the discussion of Medical Nemesis, in Chapter Seven, he was a political radical. As the Guardian newspaper wrote in a review of one of his books ‘[…] his radicalism goes out beyond Left and Right’. I’ve just been reading a short book, Math without Numbers, by Milo Beckman, and it prompts me to wonder whether, as he muses, this manifold extends infinitely along a line, or whether political cultural affiliation is more horseshoe shape than line spectrum.61 Norman Davies avers the latter, that its Left and Right extremes are close human companions, as extremes of a common radicalism. Illich’s radicalism is akin to that of Paul Tillich (1886–1965) in his description of the shaking foundations of religious belief. He was both priest and philosopher after all. His gender language is all his and he; of his age and his culture, always.
Regarding education, Illich set out his stall emphatically in Deschooling Society:
Universal education through schooling is not feasible. It would be no more feasible if it were attempted by means of alternative institutions built on the style of present schools. Neither new attitudes of teachers towards their pupils nor the proliferation of educational hardware or software (in classroom or bedroom), nor finally the attempt to expand the pedagogue’s responsibility until it engulfs his pupils’ lifetimes will deliver universal education. The current search for new educational funnels must be reversed into the search for their institutional inverse: educational webs which heighten the opportunity for each one to transform each moment of his living into one of learning, sharing, and caring.62
As with his book Medical Nemesis, which I used in Chapter Seven, I have used this book as a framework, here, because it is a perspective that challenges, not because I think it is right or wrong. Some of it rings true, some seems off-beam–on the wrong track, that is. He was an eyewitness and commentator of his times. His eleventh chapter, which I have been rediscovering, with my margin notes from that time, is about learning webs–this was from long before the World Wide Web, of course. It starts from a question he says should dominate over all others when planning educational institutions: ‘What kinds of things and people might learners want to be in contact with, in order to learn?’ He goes on to describe four kinds of educational resource. I quote here, in detail, how he introduces them:
Educational resources are usually labelled according to educators’ curricular goals. I proposed to do the contrary, to label four different approaches which enable the student to gain access to any educational resource which may help him to define and achieve his own goals:
- Reference services to educational objects–which facilitate access to things or processes used for formal learning. Some of these things can be reserved for this purpose, stored in libraries, rental agencies, the laboratories and showrooms like museums and theatres; others can be in daily use in factories, airports or on farms, but made available to students as apprentices or on off-hours.
- Skill exchanges–which permit persons to list their skills, the conditions under which they are willing to serve as models for others who want to learn these skills, and the addresses at which they can be reached.
- Peer-matching–a communications network which permits persons to describe the learning activity in which they wish to engage, in the hope of finding a partner for the inquiry.
- Reference services to educators-at-large–who can be listed in the directory giving the addresses and self-descriptions of professionals, paraprofessionals, and freelancers, along with conditions of access to their services. Such educators, as we will see, could be chosen by polling or consulting their former clients.63
What strikes one first, in this list, is its foresight of the paradigm and evolving culture of the Internet and the World Wide Web. Tim Berners-Lee had yet to start his undergraduate physics course at Oxford, five years after I had finished mine. This was the era of Arpanet and my first introduction to computer science and technology, from Peter Kirstein (1933–2020) at the London Institute of Computer Science and the first Master of Science (MSc) course in Computer Science in the University of London. The second impact of the list is more personal, in its connection with the first half of my ensuing academic career, where computer-assisted learning and self-directed learning enriched by computer-based learning resources, were key areas of experiment. What strikes me as missing–but is perhaps anticipated in the final chapter, in his recounting of the story of Pandora and Prometheus in Greek mythology and the Greek state of Plato’s Republic–is a reflection on the extent and dynamic of social change accompanying transition of formal education to a more learner directed focus; how it might unfold and be encouraged to unfold. There is no foresight of the weaknesses and vulnerabilities that might emerge within that paradigm. For example, the downside of learning in virtual classrooms–of what is lost there. He was not re-imagining education within a virtual reality, I think.
As characterizes his polemical style, Illich is strong on all that is wrong, and the need to fight for change. It is a not uncommon spirit in people fired to put right the imperfections of health care services. Such drive is a vital force in overcoming inertia. It tends to slam doors noisily and knock them off their hinges as well, sometimes! For Illich, efforts and opportunities for change are seen through a lens focused on deprivation, disadvantage and the forces that conspire to deny or limit access to education, save to those possessing wealth and power; to which one might now add luck and access to the Internet!
For Illich, modern day city life was akin to the Hell of classical mythology. For him, the story of Prometheus and the fire was a parable of how schooling had become a conditioning, creating a world in which there is great sense of expectation and little sense of hope.64 He saw the computer as amplifying that hell, saying:
The Pythia of Delphi [the Oracle] has now been replaced by a computer which hovers above panels and punch cards. The hexameters of the oracle have given way to 16-bit codes of instructions. Man the helmsman has turned the reader over to the cybernetic machine. The ultimate machine emerges to direct our destinies.65
Notwithstanding his florid apprehension of George Orwell’s 1984, and a Novacene era, it is interesting to note that fulfilment of his four wishes has been substantially enabled by the computer technology he parodied!
In wishing for something better, he wrote of education as an agent of decline in the ideal state characterized in Plato’s Republic, in which:
Man assumed responsibility for the laws under which he wanted to live and for the casting of the environment into his own image. Primitive initiation by Mother Earth into mythical life was transformed into the education (paedia) of the citizen who would feel at home in the forum. To the primitive, the world was governed by fate, fact, and necessity. By stealing fire from the gods, Prometheus turned facts into problems, called necessity into question and defied fate.66
He described modern day institutions built in this tradition as creating ‘needs faster than they can create satisfaction, and in the process of trying to meet the needs they generate, they consume the earth’, and ‘surreptitiously, reliance on institutional process has replaced dependence on personal goodwill’.67 Drawing conclusions from these Greek myths, the final paragraphs of the book are a plea for humanity to rediscover purpose, freed from the dictates and chains of status quo, and collaborating for the common good.
At this point, the Greek myth turns into hopeful prophecy because it tells us that the son of Prometheus was Deucalion, the Helmsman of the Ark who like Noah outrode the flood to become the father of a new mankind which he made from the earth with Pyrrha, the daughter of Epimetheus and Pandora. We are gaining insight into the meaning of the Pythos which Pandora brought from the gods as being the inverse of the Box: our Vessel and Ark.
We need a name for those who collaborate with their Promethean brother in the lighting of the fire and the shaping of iron, but who do so to enhance their ability to tend and care and wait upon the other.68
On reading this again, I was reminded of the altogether more satirical and subversive rewriting of stories of the Noah’s Ark, in Julian Barnes’ A History of the World in 10½ Chapters. In the first chapter, Noah is a questionable character focused on self-preservation rather than a new mankind, and the animals an exploited means to that end, rather than as citizens of a new earth.69 Barnes reveals the identity of the narrator of this story as a woodworm on board, only in the chapter’s final sentence–like a death sentence! Myth, rhetoric and satire are close bedfellows and feed from one another!
Coming back to earth, I move now to the late 1970s, when the future impact of information technology on medical education and assessment came under critical scrutiny. As with Octo Barnett’s foundational 1977 report on policy implications of medical information systems, as discussed in Chapter Seven, an early overview came from the US Congress Office of Technology Assessment. This 1979 report entitled Computer Technology in Medical Education and Assessment, which I also quoted from in Chapter Seven, brought together leaders from across acute medicine, community medicine, sociology, economics, social security, statistics, consumer affairs, health care providers and research foundations. The scope set was again a wide one, covering education and assessment and its interaction with computer-based materials. It looked at undergraduate and postgraduate training and their both formal and informal connections with patient care and life-long learning. It set these alongside changing regulatory requirements for validation and revalidation of clinical skills, considered in the context of quality of care provided–structure, process and outcome.
A key paragraph in the conclusions is as follows:
The use of computers in education assessment inevitably will be linked to their uses in medical information systems. Such linkage will allow, if not force, the formation of new relationships between segments of the medical education and assessment continuum, through the accumulation of large databases on student characteristics and performance, on physician and institutional performance in patient care, and on patient outcomes following treatment. These databases could serve as the thread of continuity between portions of the continuum. They could provide more objective and quantitative feedback mechanisms from active practice to education.70
This future-facing perspective was my rationale when seeking to connect clinical skills and informatics, as parallel themes of my first department at Bart’s, after conferment of my professorial position there. Clinical education is preparation for clinical profession, and its future thus connects directly with the previous section of the book and its focus on the future of the professions in the Information Age. I reflect on how this ambition has played out, in Chapter Nine.
The story now moves on to think about the pathway ahead for creating a care information utility, in the context of global village citizenship and evolving health care services and professional communities of practice of the future. Guided by the foregoing perspectives on the transition of knowledge and discipline, professional practice and education, how can we establish a common mission–or, at least, a common ground of mission–that evolves forward in the context and spirit of these transitions, engaging fully with future health care professionals and services, and the individuals and communities they serve?
As I describe in Chapter Nine, this landscape is already starting to assemble, through co-creation and sharing of common intellectual property, standardization of platform infrastructure and the transforming potential of personalized medicine and self-care in home and local community environments. Also, in the light of a transforming public health and societal focus that balances better between the curative, preventative and caring aspects of health care. On this new landscape, and only there, can and will crystallize care information utility of the kind that is needed–supporting better balance, continuity and governance of ways of working, on all sides. Creative commons, open platform, Globalton governance of the information infrastructure and standards and Localton governance of the information utility itself, with inclusive community ownership, participation in and leadership of the enterprise. That has been the inspiration and innovation of openEHR–it was an idea, is an experiment and is halfway to becoming a reality. Its exploratory and incremental implementation and adoption in health care organizations and communities, worldwide, is described in Chapter Eight and a Half, which gives context and evidence of progress.
Artificial Intelligence
As introduced briefly in Chapter Two, in 2019 the renowned American cardiologist, Eric Topol, published Deep Medicine.71 Microsoft Word interprets my dictation of his name as ‘Eric top hole’, and the book certainly is that! I intend no disrespect in also characterizing it as a topology of future medicine. It is an admirably articulate and thoughtful book–an extensively contextualized and deeply felt cri de coeur, grounded in both personal experience of health care and a luminary career in clinical practice and medical research, in America over the past forty years. I unfold his thinking, here. In Chapter Ten, I step back and reflect on the 2023 crescendo of concern about the impact of rapidly evolving artificial intelligence (AI) on human society, especially in the context of health care governance. Many of these fears have been imagined long ago and before the Information Age, in the writings of E. M. Forster (The Machine Stops), Aldous Huxley (Brave New World), George Orwell (1984) and in the recent novels of Ian McEwan (Machines Like Me) and Kazuo Ishiguro (Klara and the Sun). These have already surfaced at several points in the storyline of this book.
In Topol’s introduction to the book, he lays out his stall with impactful simplicity:
Now, the highest ever proportion of doctors and nurses are experiencing burnout and depression owing to their inability to provide real care to patients, which was their basis for pursuing a medical career. What’s wrong in healthcare today is that it’s missing care. That is, we generally, as doctors, don’t get to really care for patients enough. And patients don’t feel they are cared for.72
I often hear this story, and the word ‘broken’, from the front line of UK medicine, too, where my children and their friends and partners work, and from retired colleagues experiencing that world, now as patients. They have experience, and words, too, about breakdown on the patient’s side of the relationship.
Topol’s starting point for his book is bleak:
This is where we are today: patients exist in a world of insufficient data, insufficient time, insufficient context, and insufficient presence. Or as I say a world of shallow medicine.73
He nowhere minces words. Anyone thinking about the future of health care should read them and reflect. In relation to ‘Shallow Medicine’, Topol’s word cloud is both sobering and sad,74 in its panorama of patients’ two-word characterizations of their doctors. I make no comment about this; it is better to leave this to admirable doctors, like Topol.
In his Introduction, Topol characterizes his book as being ‘[…] all about finding the right balance of the patients, doctors, and machines. If we can do that–if we can exploit machines’ unique strengths to foster an improved bond between humans–we’ll have found a vital remedy for what profoundly ails medicine of today’.75 He concludes that section of the book, emphatically, saying that ‘The rise of machines has to be accompanied by heightened humaneness–with more time together, compassion, and tenderness–to make the care in health care real. To restore and promote care. Period’.76
The themes developed and examples provided throughout the book are compelling reading, placing personal experience as a patient alongside insightful professional commentary as a doctor. His story, too, conveys much personal songline. In contextualizing the advent of AI and its interaction with the nature and practice of medicine, he contrasts ‘Shallow Medicine’ with a ‘Deep Medicine’, informed by and realizing the benefits that AI already does and can, in future, increasingly bring. This he sees as improving insight that guides diagnosis, choice and effectiveness of interventions and workflow, thereby substantially relieving much of the waste and inefficiency, errors and inconsistencies, and time and money pressures that have grown to a breaking point in the Information Age. With his uniquely informed patient and clinician eye, and as a doyen of medicine’s coevolution with AI, he gives chapter by chapter examples, throughout health care, placing advances made in AI in the context of what is done today and can and could be done better with machines.
He devotes his fifth chapter to highlight new liabilities that arise in these contexts, as authority and responsibility are delegated to machines. He explores how the traditional arts of medicine, in building a trusted and attentive relationship with patients, hearing their individual stories and concerns, can be enhanced within the context of algorithms that can be more adept at discovering patterns that clarify diagnosis and guide treatment options and their effectiveness. His forthright views on the failings of Industrial Age systems and services and their wider context and cost in society are breathtakingly frank! The book is avowedly a call to arms for clinical professionals to stand up against the forces in society he sees as destroying them. He sees huge potential and imperative for reinvention of this landscape, such as in mental health, which gets a whole chapter, as does discovery science, informed by AI, which can in turn throw new light on ‘Deep Diet’ and lifestyle choices, and the way in which this knowledge can be brought directly to individual citizens.
In discussing the IBM Watson system that seeks to improve diagnostic acumen across medical practice, he is cautious and adds an impactful comment that:
There is certainly potential for computing to make a major difference, so far there has been minimal delivery on the promise. The difficulties in assembly and aggregation of the data have been underestimated, not just by Watson but all tech companies getting involved with healthcare.77
This very much mirrors my own experience of the health IT industry forays into the health care world over the past fifty years. It has provided key context and motivation of my own work in building initiatives such as openEHR and OpenEyes, and now, I hope and intend, openCare. Topol’s book is forthright in its comments about much of that industry–for example, in a punchy aside, relating a restrictive contract requiring that clinicians in institutions adopting a particular market-leading product should make no public commentary criticizing its use! Jose Collados is approvingly quoted for what Topol says is a sharp critique of lack of transparent and understandable explanation and verification of AI methods and ‘growing (often self-interested) misinformation and mystification of the field’.78
With regard to the still early days of AI, Topol quotes François Chollet, a Google deep learning specialist, saying ‘There’s no practical path from superhuman performance in thousands of narrow vertical tasks to the general intelligence and common sense of a toddler’.79 He comments that ‘It’s the combination of AI learning with key human specific features like common sense that is alluring for medicine’, and cautions that:
Progress made should not bypass the time accepted validation of the expert peer review process. Further, the majority of medical studies published to date are retrospective, performed insilico, yet to be prospectively validated in a real-world clinical setting.80
In relation to malpractice avoidance, he highlights failures of documentation and casts a critical eye over the failings of the industry’s electronic health record products.81 He is sceptical of Web-based diagnosis–noting that symptoms and signs are not binary (0-1) entities, and that ways of expressing them, and the associated body language, are important indicants not achievable in such systems.82
The book, overall, is a threefold story of Deep Medicine as a triad (Topol uses the word triad where I, as an engineer, prefer tripod, perhaps also preferring to keep feet stably on the ground and not be associated in the mind with secret society involved in organized crime!) of machine-enhanced understanding of Deep Phenotype, Deep Learning about life science and medicine and Deep Empathy in relationship of doctor and patient. Topol sees this synergy as the basis for recovery from the multiple present-day failings he describes throughout the book, which have degraded time and presence of doctors in their connection with the unique life stories and needs of their patients and achieved much less by way of successful outcomes in relation to money spent. Reading his brief mentions of the DeepMind company, I wondered what cross-fertilization there might have been, there, connecting with his evident passion for the ‘Deep’.
The final chapter of the book is entitled Deep Empathy and is headed by a quotation from my dad’s much read and pondered Aldous Huxley–as I recounted in the tour of the horizons of my bookshelves in the Introduction!
By these means we may hope to achieve not indeed a brave new world, no sort of perfectionist utopia, but the more modest and much more desirable objective- a genuinely human society.83
This chapter is once again a cri de coeur about the decline of empathy and what Deep Empathy might look like in a world where the interface of machine and AI with everyday life, and everyday medical practice, is evolving into the new era he envisages. He quotes Anatole Broyard in saying that ‘In learning to talk to his patients, the doctor may talk himself back into loving his work. He has little to lose and much to gain by letting the sick man into his heart’.84 He explores what it is to be human in this age, and what will be gained by recapturing the gifts of time and presence in the encounter with patients. His ‘Shallow Medicine’ has, he says, hugely truncated time for individual consultation, and likewise impoverished listening to patients, with clinicians finding themselves spending excessive amounts of time facing computer screens. I reflected on reading all this that his book does not address more widely the broader issue of young eyes connecting more to screens than to other eyes and minds. It is a huge topic of conversation and concern in our families. Excessive screen use in developmental years appears now to hasten myopic eyesight. We do not know what change may emerge in ‘mindsight’.
For Topol, reinvention of clinicians’ practice requires that they recover a sense of physical presence within the domain that they serve. I reflected that nursing and paramedical professions may have kept this presence more successfully than doctors, although, in my experience, they are also too often unduly beset by screens. He reflects on the changing relationship between doctor and patient in this new world and the changing priorities of medical education, matched to a culture centred more on care and less on cure.
He ends with this most heartfelt of paragraphs, once again elevating medicine as mission of care:
But it’s hard to beat the boost from a doctor or clinician you trust who can bolster your confidence that it will pass, that he or she will be with you no matter what. That you’ll be okay. That’s the human caring we desperately seek when we are sick. That’s what AI can help restore. We may never have another shot like this one. Let’s take it.85
That is why, in my world of health informatics, I have worked to help imagine, focus and create a care information utility, and openCare.
Human Connection in the Global Village
If the care information utility is to take root in a local community context, what will that community look like in the future. We are midway in transition from the Localton context of my childhood to the Globalton context of tomorrow. It is a soul-searching era–what do we want it to look like?
Important human connections have been broken and are being remade differently. ‘Company’ as a term, as Gillian Tett reminds us, derives from the Italian for the sharing of bread.86 Good company characterizes human connection. The commercial company embodied a different orientation based on money and markets, but this is also in transition, with today’s corporate identity reorientating from one centred on shareholder ownership and value, to one embracing stakeholder interest and value. Enterprise that can embrace and be co-created by a mix of citizen, community, profession, organization, industry and political stakeholders is drawn together, and balanced within the new UK legal model of the asset-locked community interest company.87
Working in the office is moving to a new balance with working at home. Health care services are also transitioning into new balance, continuity and governance, centred on the citizen and this wider and more inclusive concept and sense of community interest. We think of 2020 vision as a metaphor of balance. We are still only halfway there towards finding balance in support for the health care needs of the global village. We are unbalanced regarding lifespan and lifestyle. Not so much, now, in what we know, but rather in knowing how to use our knowledge, and deciding and being responsible for what we wish for, and what we do.
The start of my songline was as a villager in Woolton Hill, in rural Hampshire. In the 2020s, I am a retired global villager in Fleetville, on the edge of the ancient city of St Albans. This global village has shops and services way beyond those of my childhood village. In greenbelt-protected countryside just to the north is the ancient and newly planted Heartwood Forest, connected along cycle routes from Fleetville, where most of daily needs can be met within walking distance. The city centre is a mile away and a trading estate is a mile in the other direction. It is one of the busiest communities of London commuters, with trains every few minutes to London, and a partly monorail connection to Luton Airport, to the north. Covid-19 has significantly changed the scale of commuter travel to the office, with a newfound emphasis on remote work and increased activity and engagement in local community life and liveliness.
During the pandemic, local support groups have sprung up along our street and along others everywhere. Friends and family are near and far away–hundreds of miles in the UK and thousands of miles across Europe, the Americas and Africa. Some are nearby in the virtual world, and far away in the real world. Letters by post are mostly a bygone practice, almost unknown to a younger generation more familiar with communication through gifs, emojis and video-hosting platforms such as TikTok. Christmas parcels and letters have taken six weeks to cross the globe, this year. Virtual connectedness relies on an information infrastructure that we depend on and notice most in its failings or absence. Signalling failures delaying trains for hours, power cuts, gas leaks and water pipe bursts are quite rare, disorientating and disabling events. When broadband fails, it can bring life to an almost immediate halt. The electricity appetite of the Cloud is way too ravenous!
Despite the advancing media of communication and practice in the virtual world, there remain countervailing feelings of social isolation in the real world, mitigated by pets, and some say, in future, robots. It might be tempting to put this down to people getting older, but the travails of the young through the past year of pandemic that I have felt and engaged with as a grandparent, indicate that this isolation spans generations. It is interesting to see how strongly Globaltons have sought new local virtual connection during their Covid physical isolation. Isolation and polarization go hand in hand as fear gives way to anger. The adversarial, bordering on hostile, half and half, 50:50 politics of our age reflects this. Infectious and manipulable social instabilities, such as those that arose five hundred years ago, stoked by fixations with satanic practices and unleashed by the invention of the printing press, are coming into view again, today, with similar fixations, unleashed and amplified by the Internet.
Living through the uncertainty of disequilibrium is polarizing. Mervyn King describes it as radical uncertainty. Uncertainty does not preclude clarity, but lack of clarity fuels uncertainty. As Levi wrote, in Other People’s Trades, having lived through the stark inhumanity of the 1930s and wartime in Europe, humankind often reacts to uncertainty by dividing into polarized opposite groupings. Voltaire (1694–1778) wrote that uncertainty is uncomfortable, but certainty is absurd. And William Butler Yeats wrote of how in such times, ‘things fall apart; the centre cannot hold’.88 Societal polarization is about falling apart. A polarizing filter passes light according to the orientation of its component electromagnetic field. Information systems filter human knowledge and experience, according to the orientations of their creators and users, both enhancing and countering enlightenment.
And social media as an information utility is increasingly anarchic. In the sense that knowledge is information with causal power, its causal nature, both positive and negative, becomes more apparent, and its balance is brought into question. Francis Bacon (1561–1626) wrote that knowledge, itself, is power. Power is an energy and capacity; acquiring and expressing power and control in life is a vital instinct. Powerful human instinct seeks to control knowledge. Anarchy and chaos mean without form. For some, anarchy feels attractive as a rebellion and a counter against perceived arbitrary power. Other mindsets exploit and manipulate anarchy to gain and sustain arbitrary power.
But complexity does not imply chaos; the simplest of mathematical equations can exhibit chaotic solutions–some beautiful, such as the fractal Mandelbrot patterns. Living organisms are complex but life is not inherently chaotic. A living organism can and does progress through states of chaos in well-marked transitions–cell division has been described as chaotic transition. But it cannot be reverse engineered back to a previous ordered state–the two cells, remerging as one. The biochemical and physiological chaotic imbalance of sepsis can be arrested, controlled and placed in a new environment, consistent with progress towards recovery, normal function and future growth and development, allowing the imbalances to settle and be put right.
Learning is the assimilation of knowledge into the way that we do things. Learning can be a painful process. Many lives go through periods that might be described as chaotic. Some gain strength and security in surviving and coping with this adversity, and in facing and learning from the experience of personal vulnerability and insecurity that they entail. Many more cannot manage and become ill. T. S. Eliot describes April, the month of Spring and new growth, as ‘the cruellest month’.89 My dad–who throughout his ninety-four years of life battled feelings of personal inadequacy, which he attributed to both childhood poverty and lack of formal education–introduced me to that thought. His was cruel learning. He did not learn to be cruel, except a bit, perhaps, to himself, but many do.
In the Information Age, we are exploring and experiencing change and transition on every scale, from the smallest to the largest. We have acquired immense new knowledge, through observation and experiment. This knowledge holds causative power on the scale of atomic warfare, pandemic diseases and irreversible climate change. But it can be a well-marked transition, as Whitehead characterized, and our responsibility, halfway through, is to take time to understand, characterize, cope with and mark and shape it as best we can. When we are called upon to make choices, we have many options on which to place our X.
We should not trust or rely on prediction of the future as if it were a historical narrative. We must create our future in a Popperian Open Society blessed with an infinity of possible futures. The imaginative dualism of theory and experiment ties together and makes science. The practical dualism of design and implementation ties together and makes and sustains innovation. Both we describe as creative, and, as Marcus du Sautoy writes in The Creativity Code, the creativity of art and science may at some stage be exceeded by machine intelligence.90 As Weizenbaum cautioned, humane behaviour and the experience of community are at risk in the transition.91 How we guard against that is a challenge for another balance on which stable society will increasingly depend–that of private ownership and sharing of knowledge.
We need a bridge across these troubled waters of transition. Returning to etymologies, the term pontiff derives from the Latin for bridge. In contemporary connotation, it sometimes implies the hubris and bravado of pontification, positing knowledge of an uncertain, unfolding future. Building bridges combines purpose and belief, encompassing questions of where, how and why; of the science of materials and methods, design and leadership. It involves determining the optimal location for the bridge, and possessing the determination and resources to construct it and successfully cross it. And in creating the Information Society, the who is everyone–we are all bridge builders.
It is a great challenge of leadership in times of great uncertainty, to imagine, learn how to and build bridges, and lead across them. Trust in leadership is crucial and clarity and honesty are key foundations of trust. It may or may not require greatness, which is, in any case, neither born to, acquired or bestowed. It is earned and shown, not told. As Norman Davies said, for every person wanting to tell, there are twenty who do not want to hear!
To assert humanity and exhibit humility, civilized life needs three things: safe and dependable home ground and means of navigation beyond, common ground for inspiring and sharing improvement, and equitable governance whereby both local and global village citizens are participators in, and not just consumers of, the estate. This reality extends to private and corporate balance. The corporate world needs new regulation, extending beyond legal articulations of consumer interest and detriment. Democracy needs a fresh perspective and balance of rights and responsibilities. Of course, there is a lot of wreckage to stabilize in the global village and make sustainable through a new sense of ecology and ecosystem, as and when the storms and chaos of anarchic transition subside, which will take as long as it takes.
At the heart of all this for health care will be new care information utility and infrastructure–both social and technical. We need a practical sense of the form it can now start to take and how it will be created. This is the hitherto elusive ‘how’ imperative of care information utility. Information with causal power must be underpinned, justified and trusted, with clarity about method showing how it operates. It will either be democratic and led by democrats or it will be autocratic and led by autocrats and oligarchs, sometimes criminal ones! The 50:50 balance of so much political discord of the day reflects that we do not yet know where to head or whether to turn tail; we are effectively flipping a coin to decide. Policy for such an uncertain domain is almost intractably hard. In the Appendix III of the book’s additional resources, I describe what I saw of governmental implementation of the policy framework I traced in Chapter Seven, addressing the wicked problem of health care information.92 I offer this material in an Appendix because I do not wish to reflect on and critique this challenging era at this point in the story; instead, my focus here is on a different reality, of how we can now progress from where we are, towards the creation of an information utility fit for the future.
Characterization of the Care Information Utility–Perspective, Approach and Implementation
Since the early 1990s, a principal focus of my work has been directed towards realizing a coherent ecosystem of care records. Characterization of this endeavour boiled down to three interacting elements–perspective, approach and implementation. In embryonic terms, these might be termed conception, description and inscription–the framing and germination of ideas, their further elaboration and the enactment of their iterative and incremental realization in practice. Somewhat fuzzy and abstract triangulations of concerns, like this one, helped in understanding, communicating and keeping abreast of the complex balances in play. The wider context of the endeavour concerned matters of subscription–about resources, finance and governance. Who plays, who pays, and the means, rules and understandings whereby they do so. This chapter focuses mainly on perspective and approach; the next one on approach and implementation.
I summarized the status quo some years ago like this (see Figure 8.18). Much has remained essentially the same for fifty years.
Fig. 8.18 The current scene of health care computing, spanning fifty years. Image created by David Ingram (2010), CC BY-NC.

In terms of clinical effectiveness, the picture presented in the UK NHS Priorities and Planning Guidance (1996/97) is as follows:93
Fig. 8.19 The NHS clinical effectiveness drive from twenty-five years ago. Image created by David Ingram (2010), CC BY-NC.

This feels like a perspective as viewed from high up, in a helicopter; more concerned about the secondary uses of data than on its primary purposes and provenance, supportive of and building from the everyday needs of citizens and professionals, in care services on the ground. The patient feels here to be more data source than data owner–a cash cow of data serving other parties’ needs and interests. This perspective does little to help build a sense of a community that is able, enabled and trusting to use information as a utility for conducting and improving services, or to enable patients to own their personal data and participate more fully, with greater oversight should they desire it, in their encounters with the professional teams working on their behalf.
The focus of recent decades has certainly moved towards a more citizen-centred perspective and approach, as illustrated in successive policies adopted in the EU Framework Programme objectives for health care (see Figure 8.20), but with too little of the investments in national programmes directed to involving and enabling citizens to manage their health care issues more effectively, from their local and home-based environments. In this evolution, there will be much to be learned about the recording and sharing of personal data, and its governance within records of care and more widely. Transparency within this domain should not, though, be approached as a universal good. Sharing uncertain, distressing or potentially contentious health-related matters involves both personal and professional balances that must be approached sensitively on all sides, negotiated and learned.
Fig. 8.20 The contrasting perspectives of the AIM Third and Fifth Framework Programme objectives for health care–from patient as data source for systems to systems serving the needs of citizens. Image created by David Ingram (2010), CC BY-NC.

In the mid-1990s I worked closely with an innovative young hospital manager, Flemming Rosleff, who was busy transforming health care services in the Vejle Municipality in Denmark. He had read about the work I was doing for the Marie Curie Foundation with Bob Jones and Ilora Finlay, and invited Bob and me to give a talk at his hospital, about the Cancer Patients and their Families at Home videodisc educational resource we had developed together.94 Flemming subsequently worked as a management consultant for Coopers and Lybrand in London. He wrote an influential report on managed care systems in Europe, in which he identified the need for a new generation of information systems to support services.95 This is the scope he set out there (see Figure 8.21). This, too, has the flavour of a helicopter perspective. We might now think of the challenge also from a perspective of self-management of care.
Fig. 8.21 Flemming Rosleff’s definition of managed care. Image created by David Ingram (2010), CC BY-NC.
The following sections are about the values and principles framing the information systems that this would require and the mode of their standardization. They need to be based on common ground that provides scope to accommodate diversity of individual need, preference and choice, and foster innovation, as opportunities arise, and times change. The more simply the choices facing citizens are identified, the more likely they are to be communicated, weighed and acted on effectively. At the centre of this common ground is the care record. Its principal stakeholders are patients and their families, and the professional teams they connect with in their care. Other records and resources, centred in many associated institutions and industries, will connect with this common ground, both to supply data captured in the record, and make wider use of it.
Values
Our culture and the human values we subscribe to say who we are and are central to our human connections and what matters to us. The governance of the care information utility must reflect and be inclusive of all who create, operate and depend on it–this is the only way to grow and maintain mutual trust, which is what matters most. Communities that realize and sustain the utility will need to see themselves as being locally centred and globally integrated. They will share methods globally and customize and deploy them in line with local needs. Their culture should be one that thinks for itself and has self-belief. The utility will have fractal connectivity in two directions–from the individual citizen connecting within health care systems and services, locally and globally, and from each global component of these systems, ramifying to each individual citizen, locally. These twin perspectives are anchored within common ground of shared knowledge, method, environment and community.
It is in the relationship of the two perspectives that we struggle to achieve balance, continuity and governance of services, and make them mutually coherent. Where they are not coherent, their computational counterparts–the artefacts separately implemented in many parts of the information ecosystem, to address needs perceived there–will reflect this incoherence and amplify its confusions. In the Information Age, actors in different businesses, institutions, professions, voluntary services and local and national governments, have all, individually, invented and propagated information appliances and systems according to their own take on the semantics of the domain they connect with and the purposes to be served. Taken together, they are assembling, albeit largely unwittingly, a non-coherent and tottering data and computational tower of Babel. A new culture of community enterprise must start to deconstruct and reconstruct this reality and build towards an information utility based on common ground of human meaning and computational semantics, whereby people can communicate safely and effectively, with and through the computational web.
Three quotations characterize the energy and approach required within such community if it is to succeed. They resonate with culture and values more generally.
The ultimate hidden truth of the world is that it is something we make and could just as easily make differently.96
This is about self-belief and self-reliance. We all make health care–looking after ourselves and those we care for, and in relationship with those who care for us: family, friends, community and professions. We own our personal health care needs. People given trusted and shared means and methods to connect with one another, in meeting their own and other peoples’ needs, are every day inspired with energy to do so productively.
We may become the makers of our fate when we have ceased to pose as its prophets.97
This is about realism in the here and now and avoidance of hubris and pretence of knowledge in prediction of the future. We should attend to making and doing what needs making and doing now and prepare, as best we can, for a future that is unknown and unpredictable.
In the end, therefore, intellectual definitions raise more questions than they answer. It is the same with European history. As with a camel the practical approach is not to try and define it but to describe it.98
This is caution against burrowing too deeply, hedgehog-like, into the fractal complexity of current anarchic realities, but to stay more straightforwardly focused on the simpler elements that can provide traction in meeting health care needs. We should accept that the present transition into the Information Society is complex and anarchic–we should observe and describe it and not attempt, too much, to define it. Describing and defining go hand in hand in theory and experiment of science. In social matters, we learn to cope with, as well as describe, the here and now, before we can reasonably know how to rationalize, shape and manage the unfolding future. The quotation is in tune with Mervyn King’s reflection that managing complexity of the world financial system should focus on telling stories that assist in coping with it, as much as in predicting and shaping it. They are both arguing for a more human balance of hand and head. Norman Davies also wrote Heart of Europe: A Short History of Poland, alluding to heart as culture and soul, as well as central location.99
It would be interesting to have heard the thoughts of Illich about the culture of transition of society in the Information Age. In the prospectus for Medical Nemesis, he argued that the principal challenge in health care is a human challenge of recovering and reinstituting human autonomy and pursuing health as a human task and virtue. He described it as a ‘rediscovery’ that effective health care depends on self-care. Concerned by what he saw as ‘iatrogenic disease’ arising from the practice of medicine, his diagnosis was that an over-dependence on medical oversight was ultimately disabling, turning humankind into lifelong patients. He proposed legislation that would rebalance society towards autonomy and self-care, and away from an industrial culture built on the medicalization of life. He even proposed to outlaw all technology that could not be operated in the hands of lay people–a trifle exuberant, perhaps–truly, a folk medicine of the Information Age!
Leaving the more ideological aside, one might observe that in the changed scientific and technological landscape of the Information Age, the evolving pattern of health care services has recognized and adjusted to much of the reality that underlay Illich’s observation and perspective of fifty years ago. He was a Tillich-like figure, seeking to shake the foundations of orthodoxy in medical practice, in the way that Tillich described the shaking foundations of religious belief–a nice conjunction of names and missions! Likewise, in Deschooling Society, his perspective of education was built on autonomy of the life-long learner. His advocacy was for technology-driven learning webs, within which learners and their teachers could communicate and be informed, beyond the constraints and manipulations he identified with schooling institutions and their governance. Although richly polemical, it succeeded in anticipating and addressing contemporary concerns of today, as such technology and method reveal themselves, and their benefits and limitations unfold more widely, including in the health care of our changing times.
Coping is an essential frontline strategy for anarchic times. Coping is frontline in health care. If autonomous citizens are to be co-creators with professionals of their health care, and participate in maintaining its balance and continuity, under a co-created governance arrangement, they must have the option and wherewithal to manage their health care as much as they are able, prepared and wish to do so, and to be supported, as far as possible, when in need.
To envisage information systems with all this in mind is not to say that health care services could or would be organized and enacted in a spirit of ‘you’re on your own, Jack’. It will, rather, reflect the requirements of community wherein patients and their advocates can connect with professionals and services, protecting personal autonomy and sharing roles and resources in ways that are negotiated and agreed as balanced and equitable on both sides, and embodied in clear and stable governance arrangements. It will require ways of working that embody fairness in the balance of rights and responsibilities–of both givers and receivers.
Where we fail adequately to cope with the changing cultural dimensions of balance, continuity and governance of health care, computerization will further exacerbate difficulties. Load the rifles with computer-enabled silver bullets, and use them to kill disease, but do not expect this to clear the fog (elision of fox and hedgehog, remember!) of confusion caused by computerization of the imbalance, discontinuity and governance mayhem of unequal and inequitable health care services. They will evaporate some of it and add to it elsewhere, as they explode!
Principles
Principles are the basis on which we start to implement on a blank canvas and martial our ideas. Mine start from experience and observation that information systems of today are costing too much, delivering too little of the value they could, and are too slow in adapting to changing needs and opportunities. With the evolution of technology over the past thirty years, and alignment of software methods and standards to the emergence of the Internet, there is, for the first time, a sound and sustainable basis for transition to an information utility for health care, that will work and deliver value for citizens and assist in improving the working life of professionals. There is, however, a considerable legacy of software and systems that will not survive the transition and is impeding it.
The challenge is now of working incrementally to supplant this legacy with a sustainable and future-facing resource. The community that comes together around this mission should think big but start small, focusing on demonstrably achievable, safe and incrementally implementable goals, with iterative review. It is a huge endeavour but there is a huge human resource to engage with in this, including very capable and motivated computer science students eager to participate in work that they see to be of transforming value. Catalyzing this engagement requires a coherent platform and method available for all to learn about and work with, and a mature and joined up community of practice to join in with.100 Big Data encourages and excites big ego. The information utility should be built stepwise from Little Data, the term I alighted on, many years ago, for the ‘omnuscles’ of clinical data of Chapter Three. A Sunday Times review of data technology that I read yesterday (February 2022) highlighted the risk in applying AI methods to poor quality data.
The principles that should govern future care information utility are gradually clarifying along the following lines:
- An information utility placing the citizen and the data and resources they command at the centre of architecture and design, with open governance that protects their ownership and autonomy;
- This utility should be run as a public enterprise with commercial partnership enabling innovation within a common framework, built on top of the World Wide Web Consortium (W3C). Public enterprise across countries should combine their efforts to fund this platform. Revenue from use and exploitation should be invested back into its ongoing development and support;
- The platform specification should maintain vendor and technology neutrality and be owned in the public domain, designed to prevent antitrust outgunning trust, through monopoly and appropriation of intellectual property;
- Data used in commercial context should protect the IP of the owner of the data and require that revenue be shared equitably to provide resource for the support of the utility;
- Choice and shaping of content should emphasize support for balance, continuity and governance of health care services more broadly. The following linked tripods of concerns are central to these:
- Citizen, professional and organizational requirements;
- Service delivery, education and research needs;
- Technical rigour of implementation, engagement and participation of users, and public trust;
- Patient autonomy, professional peer review and external audit and review;
- Implementation of systems and services should emphasize coherence, efficiency, and simplicity:
- Generic methods and standards supporting design, implementation and sustainability of systems;
- Interoperability of data and algorithm, enabling balance of knowledge and reasoning, observation and measurement, modelling, mathematical and logic-based analysis and information engineering;
- Scalability of data capture, storage and computation, from personal information appliances and local networks to grids of processors and storage devices;
- Efficiency of storage and retrieval from sparse, changing, and accumulating arrays of data, in the different contexts of personal, professional and population level usage;
- Unified and secure user interface with balance of client-side and server-side processing and high bandwidth connectivity throughout.
Whatever the principles adopted, there must be contracts and there will be consequences, accordingly. These will be social contracts as much as commercial contracts. Often the following of more than one path, in parallel, can be a sensible risk management as well as leading to a symbiosis that proves more useful than following just one.
Culture, values and principles must cohere within an approach to creating an integrated and sustainable information utility. Following the wisdom of Fred Brooks, computer systems need architects who oversee their design and implementation. This is a creative role and needs something to start from, against which to test principles and ideas about ways to go forward. My first attempt to capture the architecture of health records was in 1991, when formulating the GEHR project that was commissioned by the EU to propose a common architecture for health records. This story is told in Chapter Eight and a Half, and in Chapter Nine the story moves on to consider a similar exercise in the context of the wider care information utility.
Now, thirty years on, the original GEHR architecture has substantially evolved. In continued fulfilment of its founding principles, it is openly specified, instantiated and widely implemented, in different software technologies and by different vendors of systems, under the aegis, now, of the openEHR Foundation and the self-governing openEHR International Community Interest Company. The need is for a similarly cohesive and concise, principled framing of an architecture of care information utility, centred on common ground of the care record.
A note of caution seems appropriate at this point. As recounted in the context of Illich and his book Deschooling Society, sickness and death were Zeus’s vengeful legacy, willed to the world. In the myth, sickness and death betoken all manner of evils that the gods bestowed. They have come to dominate health care systems and, in Illich’s perspective, led to over medicalization of society and its expectations. The computer as Pandora’s box and information as that released from it into the world, is tempting analogy or parable for our times! The legend of Epimetheus (whose name translates, Illich says, as afterthought) reflects the need to be careful about what we wish for. Rescue services have a hard job. It is a hard job when we are left to contain and reverse floods and put out fires. It is a hard job to rescue information when it has spread into the environment, as a sickness rather than as a utility. The legend foretold trouble, and that we certainly have. It has picked up a redemptive flavour of wisdom arising from folly. Erasmus used it to illustrate a Latin proverb, Malo accepto stultus sapit [from experiencing trouble a fool is made wise].
Are we yet wiser? The Information Age has had its grand follies and a lot of money has been parted from foolish owners along the way. Taken to extremes, information, information, everywhere, and not a pearl of wisdom in sight! A bit like King’s pithy advance on Samuel Taylor Coleridge (1732–1834) and The Rime of the Ancient Mariner, saying of the alchemy of money: ‘debtors, debtors everywhere, and not a loss in sight’.101 The goal of care information utility is to provide a connective and integrative role, at one with human wishes and wisdom, and to guard against fragmenting influences that unleash new troubles to beset future generations who live on into the Information Society.
Standards and Standardization
Communication of any kind of information involves considerations of trust. How far can we trust that measurements of weight, length, time or anything else we choose to measure, that arise from different devices, in different locations and contexts, that are declared to be comparable, are in fact comparable and not subject to what might prove significantly different bias and noise?
One way to feel sure might be to place the devices used, side by side, and trust one’s own sense that they are recording the same measurement of a common object, as one makes the measurements. That may once have sufficed, but to most intents and purposes, today, it is not a practical solution. Another is to calibrate the different devices and methods that are used to make the measurements in the different locations, against a special status device or object that is declared to be the faithful representation or measurer of the quality being observed and measured. Then, if each of the other devices is shown in this calibration process to measure identically with the special status device, or within a prescribed narrow range of agreement, we may satisfy ourselves that they can each be trusted, independently, in different locations but otherwise reliably similar contexts, to be making acceptably correct and comparable measurements.
That special status device or object is the ‘standard’–a standard object of weight (e.g., one kilogram) or length (e.g., one metre), or a standard device for recording time in seconds, for example. It might be called a reference standard as all objects or devices used in measurement are calibrated and referenced to this one, when justifying and stating their credentials as a trusted means of measurement. Clinical chemistry measurement was an early field where improved standardization of devices and methods was imperative, to ensure dependable accuracy and reproducibility of blood and other clinical test results obtained in different laboratories, using different methods and machines. Standardization became central to their quality assurance programmes.
Systems of standardization pervade throughout science. They vary according to geography and discipline, and within discipline. Converting measurements between different standardized units was mental arithmetic exercise in my primary school maths classes and tests (weights in stones, pounds and ounces to grams, and lengths in inches, feet, yards, chains, furlongs and miles to metres). Standards now permeate and prevail more widely, into ways of doing things as well as ways of measuring them–a standard glucose tolerance test procedure, for example, defining the fasting protocol, administration of the bolus of glucose and collection of subsequent blood samples and measurement of their glucose levels. They permeate into standard ways of recording and communicating information. People train in their use and their skills are assessed and accredited accordingly.
In the early days of my encounter with computer systems, device manufacturers set their own standards for the electrical signals and data formats employed in devices connected to the computer. Analogue and then digital signals communicated between device and computer, making the connections. Computer manufacturers wrote software to manage these transfers and called them ‘device handlers’. The scientists and engineers who were developing their own devices and interfacing them to computers, were on their own. The computer manufacturer gave instructions on what the computer needed to see, both in terms of hardware plugged directly into its internal data highways, and hardware connected via manufacturer-provided generic modules connected to that highway, that received or generated analogue and digital streams of data through which device and computer were to interact. The developers created these bridging electronic circuits, adjusting device and software to make the transfer work correctly and efficiently.
In my early work in medical physics, our team designed electronic circuits and wrote machine code software to transfer and process data from imaging devices, to and fro, across these electronic bridges between device and computer. In time, their design and manufacture took advantage of commoditized electronic components one could buy off the shelf–integrated circuits and modules such as analogue to digital and digital to analogue signal converters. These interface circuits and algorithms developed to process the signals and data generated by them, became integrated within commoditized specialized hardware and software modules. Devices took on some of the work previously handled by the computer, and vice versa. The physics and electrical engineering discipline involved in working with these devices became standard working practice for their users, but the standards defining the operation of the devices–what went into them and what came out of them–were specifications determined and supported by their manufacturers. The user selected the product device that worked best in their situation, and that was all that was possible and mattered.
For connections at a distance and between different users of the computer systems, there were limited options–twisted-pair cables enabled signals to get there and be disentangled from noise picked up along the way. Coaxial cables transmitted the signal along a central wire and provided encircling shielding. There were horses for courses, and you had to know about electrical circuits, amplifiers, filters and earthing differences between buildings, that might cause potentially disrupting electrical current flow, and the like. There was common ground with the then current technology of analogue telephony and its connecting lines were used to piggy-back the signals from devices to computers and then across the public telephone network. Binary Morse code had long been transmitted by hand-operated switching of analogue signal levels along telegraph lines, but this was no way to transfer rapidly alternating signals of the bit streams of digital data! Neither could one route the data automatically, through a manually operated telephone switchboard. Automatic switching arrived, with new issues for enabling and ensuring smooth connection of a continuous signal through exchanges, like keeping trains running smoothly on railway lines routed through railway networks.
The problem then became that of the Portbou rail interchange between France and Spain. Different telephony companies were not in a position to call the shots over their competitors. Even conquering armies, as recorded by Norman Davies, had trouble in coordinating standards of munitions and firearms, as vanquished armies were shotgun-wedded with their victorious counterparts! Industries had to cooperate to enable signals to flow between their respective domains of sovereignty. Circuits could be arranged to convert electrical signals between proprietary standards, but at a cost of extra equipment and degradation of the signal–less signal, more noise. The industries had to cooperate, in order both to create and evolve their markets and to compete. If they could agree on a common standard for the transmission of signal between their respective domains, additional cost and loss of quality could be avoided. Conformance to a standard was an advantage for them–of course they fought over what that standard should be! Oftentimes, unsurprisingly, corporate muscle and preservation of status quo, would vie with objective appraisal of technical superiority and experience in use of competing putative standards. More powerful customers and users wanted better and cheaper services and began to insist on standards, too, as these started to impinge on aspects of their own operations and viability.
The problem of standardization mutated and moved on. Not just the electrical engineering of the route but managing the traffic. Trains on railways are controlled by signal boxes and procedures that avoid collisions. I can still remember steam train drivers passing a huge metal token between them, as one completed transit along a single-track section of line in one direction and the other waited to be allowed to enter that track in the opposite direction. The driver in possession of the token was the only one allowed to take their train along the line. Putting more and faster trains on a network of lines brings risk of accident–breakdown of trains and breakage of lines, blockages disrupting flow, and collisions of trains. In digital networks, data traffic management arrived–embodied in protocols for detecting and recovering from collisions and errors and accidents that crept in along the route. These provided ways of grouping bit streams together within blocks of data, and blocks within messages, all electronically tagged and labelled, such that the structure was intelligible all along the line. These were matters of the technical framing and transmission of messages. The meaning of the message was immaterial to its transmission–it could be a birthday greeting or an urgently needed clinical laboratory measurement, everything went along the same lines and conformed to the same underlying standard pattern.
And by this stage, there was a hierarchy of different levels of connection involved in the communication, all of which were potential circuit breakers, combined and described in the language of performance: efficiency, effectiveness, cost and risk. Mathematics, physics, electrical engineering, computer science and human experience and skill were all in this loop, all adapting to one another in providing utility of the communication. And their component contributions were interdependent–broken or heat-buckled rails, snow or leaves on the railway line, absent signal box operators, broken levers and wires, company bankruptcy. There was need for a protocol of mitigations to minimize their impact. Complex socio-technical systems emerged, where the whole was no longer simply the sum of its parts but developed its own behaviours and was embedded with the purpose and meaning of the information being communicated. Human communication interwove with technical characteristics of the communication system.
And so, in health care and medical computing, our eyes focused on standards. Signal protocols led on into network protocols, message protocols, document markup methods, health care messages, clinical terminologies and classifications, protocols of health care processes, audit and management, regional and global information standards and the top to the bottom of the World Wide Web. The terminology and acronyms of this world buzzed with feedback resonance of loops of communication: (in no particular order!) Ethernet, TCP/IP, OSI, HTTP, EDIFACT, SGML, XML, HL7v2, HL7v3, HL7 FHIR, IHE, ICD, Read Codes, GALEN, SNOMED, ICPC, LOINC, Casemix, HRG, DRG, CBS, GEHR, Riche, LRA, openEHR, CEN/ISO 13606, W3C, OMG…
OMG (Object Management Group) is an amusingly apt acronym and emoticon to complete the Topsy-like proliferation and complexity of these standards! ‘Twitter’ is apt as a characterization of the messaging and communication about them! These domains of standardization did not necessarily work well, or at all, together. Conversions diminish signal and aggravate noise. The Portbou interchange slows transport flow and aggravates noisy passengers! Families of standards linked arms and repelled invaders. De jure battled de facto. There was accommodation to the impasse. Neither France nor Spain was going to completely re-lay its railway network and change all its trains.
As users, most people are mainly concerned with the performance of the systems they use. Could my wife’s ninety-six-year-old dad hear her across the mobile and landline telephony network connecting between her mouth and his ear, in England and Poland? Some users may be consumed by dislike of the colour of the telecom maintenance engineer’s company van, and judge his service accordingly, but, hopefully, only a few! In communication about health care–and Bożena and her dad were talking doctor to doctor, as well as daughter to father, and they trained and practised in different eras, in different specialties–communication of meaning is of a different order, and technical and data-driven standards at that level still have a long way to go. They will be central to care information utility.
The story of information in the context of telecommunications of the Information Age is an interesting allegory of the story of information in the context of living systems that I sketched out in Chapter Six. That story traversed from the machinery of life to the function of the integrative nervous system, information networks of living cells, organs, bodies, conscious thought and meaning. The science of life has tunnelled down to the bioenergetics of electrons and protons acting across membranes and the free energy donations from the sun. The science and engineering of information has evolved from statistical physics of gases and electromagnetism, through the engineering of circuits, the capture and communication of signals and messages, to the exchange of records within health care systems and information utility.
The purpose of a railway system has definable technological, personal, social, economic and political contexts. The purpose and form of the health care systems has been turned upside down in all these contexts in the Information Age. I am not, here, doing a Horst Rittel (1930–90) and Melvin Webber (1920–2006)-like categorization of ‘tame’ and ‘wicked’ problems, morphing into them being labelled as ‘easy’ and ‘hard’. I am highlighting meaning and context as being more tangible and tractable matters to judge and decide on for a railway, than they are for a health care system.
Health care information infrastructure has, however, grown like a railway or telephony system, emphasizing the purposes most suited to machine and management and relegating those aspects more dependent on human meaning, skill and judgement. As our focus necessarily now moves above the machinery of the infrastructure to its purpose and performance in achieving desired outcomes, we move up a level, from data model to information and knowledge model, and how they support connections of meaning, context, workflow and reasoning. The quest for care information utility is challenging boundaries of connection and communication–in research, education, professional practice and in personal identity and autonomy. The nature of signal source, message, route, and destination, within the infrastructure, then assumes a place within meanings and contexts of information utility. That utility is intrinsically much harder to standardize and reengineer than a telephony or railway system, in large part because it is abstract and cannot be seen. Health System Standardization is HS2 as opposed to HS2–the current project for a high-speed railway joining London and the North of England!
The standardization of data and computer systems that work and can be sustained through periods of rapid clinical and technological change, over time, is, for all these foregoing reasons, a very considerable challenge. The quest for this standardization has been both the albatross and Achilles’ heel of NHS IT programmes, throughout my five decades of involvement. It has been labelled, but gone unrecognized in nature and form, for too long. This is especially important because, in many circles, a health care standard is seen as an enforced technical conformity of systems, as opposed to its primary purpose, which is as a lingua franca enabling and facilitating communication about meaning. This, like any language, evolves over time, as clinical practice, science and technology move forward. But therein lies the rub. For some, control of such standards is an important insurance policy guaranteeing marketability of products and services. Standards are fought over and defended, becoming like tablets of stone, because software costs money and changes in underlying standards can rapidly render systems unmarketable, unsustainable and obsolete. That is a bit like the Académie Française enforcing rules of usage to tell the French people how to speak proper French!
In recent decades, the difficulty of keeping pace with changing technology, both hardware and software, at scale, within large health systems has proved unmanageable and unaffordable within the parameters set for them. So much so that the field has, in the main, been characterized by local successes–local, that is, to a particular technology, domain or institution delivering services–and costly global failures–global, that is, in terms of sharing records across domains in which the data about a particular patient needs to be communicated and worked on, wherever, whenever and by whoever they are cared for, locally, nationally or, increasingly, internationally. This is in the context of capture, processing and communication of data where patients, themselves, are more closely involved, or need to be able to be so involved, when at home, out and about or travelling abroad.
New approaches and experiments are needed to meet the challenge of defining a practical and deliverable scope for standardization of health care information as a utility. These need to focus on working more effectively and practically, with patients, professionals, health care providers, education, research and industry, to learn, through practical implementation experience, about standards that work. The evidence and experience of past endeavour is that the need and urgency of this goal is recognized but the means of framing and implementing it has proved beyond the joined-up capabilities of the teams and environments in which it has been pursued.
As a result, our options when buying IT are too often locked down in inflexible designs, which cannot be changed because their technological underpinnings are already effectively obsolete, or where there has been so great a past investment committed in them, that it is deemed impossible to consider experimenting and replacing them with new methods and approaches. That is why innovation and implementation to get past this impasse is best and most achievably envisaged at smaller scales of endeavour, with agile and incremental integration, outwards and upwards, from there.
Some levels of standardization matter greatly as means for underpinning coherent, efficient, safe and effective information systems, and creating stable and transparent markets for those that develop and trade in them. They reflect cooperation that underpins and makes possible competition, while leaving opportunity for commercial gain where value is added through private investment. There are issues of equity and regulation, ethics and law, and human roles and responsibilities, that favour basing standardization of the specifications, methods and tooling required to underpin and support a coherent care information utility, on common ground and under Creative Commons and open-source licensing. I address these issues in Chapter Nine.
Standards presenting as open commons are, inevitably, sometimes manipulated behind the scenes, to facilitate new enclosure, through undercover relationship with vested interests that are pitching to take special advantage. Standardization processes are, as ever, high politics and hard grind. I have observed international standards processes at close quarters but not engaged much in the circus they often seem to bring. They are greatly needed but come at a price. They would be better and more authentically handled from a more experimental and evolutionary perspective, based on implementations as well as designs. Standards upholding quality of health care and the engineering of its care information utility cannot be justified on the basis of political compromise–such standards are Emperors’ clothes.
Many areas of the technology and software of health information systems have achieved official or de facto status of standards over my songline. Standards help to stabilize and consolidate markets, and, as I have said, they are also managed and manipulated to the advantage of different competing interest groups. Apple operates an ecosystem for its products and an associated App market that aligns with its proprietorial rights in iOS. Google has adopted Android as an open-source platform for hosting Apps. In health care, free market monopolist tails must not be allowed to wag dogs and create fogs obscuring what should be coherent community wide interest. Once again, balance, continuity and governance are important litmus tests of how such evolution of platform and utility is to be regulated.
Parenthesis–What Matters and Why
If we are not satisfied with the continuation of the Chapter Seven rush to find gold at the end of a rainbow in the Information Society, and do not wish to solely rely on chance to determine the outcome, we need to be clear about what we want to create, and why. What are the key considerations guiding our approach to making the care information utility fit for purpose in the Information Society, and why are these the key considerations? What cultures, values and principles, missions, goals, methods, teams, communities and governance do we seek? All of these will be inherent in charting a path and we need them to be, so far as possible, mutually coherent and sustainable. Because otherwise, the computer will do for us what it is has shown itself good at doing–exposing and further burdening us with the inadequacy and incoherence of our ideas and actions. And we must not delay this work. Lacking coherently implementable and implemented policy, each year we generate new, disjointed legacies that become ever harder and costlier to dislodge. These are two good reasons why.
Chapter Seven surveyed fifty years of policy perambulation. Chapter Eight has suggested a new policy focus–the Care Information Utility. Chapter Eight and a Half now describes movements dedicated to iterative and incremental exploratory steps in this direction, designing and implementing standardized clinician- and user-governed clinical data models and a related information platform architecture, supporting coherent care records. It shows how it can and is being done. Chapter Nine is about how to learn and evolve from this work to implement and sustain a wider care information utility, and create the environments, teams, leadership and governance required to that end.
As I first made notes for this section, the Covid-19 pandemic had been evolving for a year and was currently declining from a precipitate third wave peak after Christmas celebrations, into early 2021. My reflections on this chapter reflect the dramatic community context of that time. What was seeded mainly in the South-East and spread north westwards, bounced back, with upsurge in the North-West spreading in a south-easterly direction. Pandemics flow like waves and jump long distances, like tsunamis and grasshoppers. And viruses mutate, posing new challenges of detection, measurement, prediction, containment and treatment of infection. A more highly infectious mutant form emerged in Kent and rapidly dominated a third wave of infections, spreading northwards again. And successful vaccine trials led to a national mobilization of vaccination, centred in local communities, and resulting in half the adult population being vaccinated within three months. Further resistant strains were spreading from South Africa and Brazil and causing increasing alarm, with calls for heightened restrictions on travel, just as summer holidays to warmer climes had started to look feasible, once again.
Our Globalton village had seen relatively few cases, thus far, but the pattern of infection was complex. It changed rapidly, within and between adjacent areas of the country. As everywhere, our community was greatly affected by the restrictions, evoking many daily acts of kindness and support for those shielding at home, orchestrated through social media groups and in the Street, City, County and Country. The challenges, responses and impacts varied greatly across the country and across the world. There was a Pandora’s box of uncertain unfolding outcomes.
For those of us who knew and remembered it, this felt like a resurgence of Localton community connection and sense of belonging–not starry eyed but with a stability and certainty no longer so widely felt. It has been an encouraging and optimistic revelation and experience of what, in my childhood and early decades, people remembered nostalgically as wartime spirit. It is often called team spirit–successful teams, in work and sport, or anything else, share a common sense of occasion and purpose that overrides common seeds of fragmentation and distrust. It is an emergent phenomenon–spirit engenders success and success engenders spirit. It is a dynamic of head, hand and heart and people care about those in their teams and are cared for by them.
This care is a local phenomenon, but it spreads outwards and upwards. Neighbourhood relationships, so often busily constrained behind front doors and morning rushes to schools, cars and trains, opened into neighbourly care and concern, along streets and within communities. It has been in evidence when industry and academia have applied hands to ploughs, with rapid cooperative and collaborative effort to create new vaccines and ventilators, moving from prototype towards production and testing, with unheard of combinations of twenty-four-hour skill, diligence and speed. And it has been on show in the military mobilization to create huge fallback hospital capacity and in organization of the vaccination programme. Above all, it has been in evidence in extraordinarily demanding commitment of frontline staff, who are the most exposed to infection in the epidemic.
We must not get carried away with euphoric relief that some anxious early forebodings of worst outcomes were forestalled in this way. The capacity to rework hospital care patterns to absorb a huge influx of seriously ill patients, where the disease presenting was a largely unknown quantity, has impressed, as seen from the outside, and exhausted those working on the inside of those services. Reading the very moving diaries written, by their attending nurses, for patients near to death and in induced coma, one can feel the presence of dedication and care. Moving accounts of care for residents of care homes abound, as do accounts of families coping with the abrupt upending of their lives, with loved ones suddenly stricken and in prolonged intensive care and dying.
But the Covid-19 pandemic challenge to health care, nationally, has also highlighted crisis in care services, locally. It might be characterized in terms of how priorities were set for testing for the disease and availability of safe working contexts for staff, including protective clothing. The unmonitored spread of asymptomatic infection in the community and into the care sector was disabling and created a surge of deaths of people who should not have died at that time. The movement of infected but untested patients from highly infected hospitals to then uninfected care homes, also created high risk of outbreaks there. There was a bifurcation of attitudes. Those who were unaffected and perceived themselves as having minimal risk wished to plough on. Those who were affected and at highest risk, and those in the front line of services struggling to cope, sought caution. The balance struck was political and chaotic, and the cost has carried forward and been prolonged, in the country’s account. John Houghton (1931–2020) spoke of present disaster as the only driver of change in society. Global pandemic, like irreversible climate change, is a shock and call to action, where we are confronted to find common ground on questions about what matters and why.
The Covid pandemic is a partial metaphor for information pandemic, which has been accelerating, chaotically and expensively, through the information revolution of the past seventy-five years, starting from the time of foundation of the NHS. This pandemic has co-evolved alongside changing science and technology but remains substantially unbalanced and uncontained. If you doubt that, look again at the perspectives and policy goals of the 1970s and those of today, in the sequence of documents I reviewed in Chapter Seven. Couching these in new language does not alter their essence.
The experience of going through the Covid pandemic gives pause for thought about lessons learned from the information pandemic, and how creating a more coherent information utility could in some sense vaccinate us against its harmful effects. There are three key issues which stem from an understanding of the nature of information utility. It is an organic entity: a tree that needs to be seeded and nurtured, as much as produced and sold. It cannot be created and imposed, it needs to take root and grow. The value it represents derives from its existence and how it is created, sustained and trusted, as much as from what it is. It has no meaning standing alone; it needs consensus, effort, business model and incentive to integrate coherently with citizens and their health care in everyday life.
Thus far in the book, I have explored numbers of ‘What is’ questions, starting from basics like ‘What is reality?’ and ‘What is life?’; to this list we have now added ‘What is the information utility for health care?’ There then follow all-important ‘How?’, ‘Who?’, ‘Where?’ and ‘When?’ questions. How is the care information utility to be imagined, designed, created and sustained? And who will do this work and where? When is easier–best to start now! Different approaches to governance of such endeavour have reflected differences of culture and belief. Leaving aside coercion, they mirror the classical advice of Confucius (551 BCE–479 BCE), that to govern there must be trust, food and weapons and the greatest of these is trust. By analogy, we might equate them as follows to a successful campaign against Covid-19:
- Trust = fairness, openness and humility;
- Food = treatments, vaccines and information;
- Weapons = people, resource, infrastructure and method.
In tackling the challenge of information utility, the food is information and the trust and weapons are much the same. As the Susskinds summarized at the end of their book about transforming the professions to be fit for the Information Society, the question is whether there is the will to do it. ‘Where there is a will, there is a way’, is not so true of the Information Age. The nature of government and the weapons at its disposal have changed or are at least changing. To govern is to enable good governance and a weapon is a means to an end. Where there is seen to be a way, it is more possible to summon the will to do it–there is little will for an untrusted or untested way. The way is about how, and that is about method–and it is to this question that the story now moves in the first half of Chapter Nine. Before that, Chapter Eight and a Half, mirroring that of Barnes’s A History of the World in 10½ Chapters, is a parenthetical trip along the timeline of my work of thirty years discovering care information utility. This then naturally raises two further questions: ‘Who?’ and ‘Where?’ The next sections of Chapter Nine are about people who take up the challenge of creating and sustaining care information utility, and their leadership in the environments created for this work. The story concludes in Chapter Ten, with a discussion of what remains only half done, and the Postscript forms a preface to the second half, in whatever comes next.
1 Adventures of Ideas (New York: Macmillan, 1933), p. 246.
2 E. Topol, Deep Medicine: How Artificial Intelligence Can Make Healthcare Human Again (London: Hachette, 2019), p. 31.
3 On the Aboriginal concept of the Dreaming, see Preface.
4 General Medical Council, Tomorrow’s Doctors: Recommendations on Undergraduate Medical Education (London: GMC, 1993).
5 M. C. Escher, ‘Ascending and Descending’, Digital Commonwealth, https://ark.digitalcommonwealth.org/ark:/50959/3r076s51v
6 On this Polish expression, see Preface.
7 R. D. Putnam, The Upswing: How America Came Together a Century Ago and How We Can Do It Again (London: Simon and Schuster, 2020).
8 Having first written this chapter in autumn 2020, I later discovered and read Suzanne Simard’s wonderful book, published in May 2021, entitled Finding the Mother Tree: Uncovering the Wisdom and Intelligence of the Forest (London: Penguin Books, 2021). This is a story about the forest ecosystem, based on her experience and foundational research of several decades, from childhood in a family and community of foresters in British Columbia to her status now as a world authority on forestry. I describe it further in the section below. I, too, grew up in remote countryside, amidst woods and trees.
10 R. E. Susskind and D. Susskind, The Future of the Professions: How Technology Will Transform the Work of Human Experts (Oxford: Oxford University Press, 2015), p. 307.
11 J. Weizenbaum, Computer Power and Human Reason: From Judgment to Calculation (Harmondsworth: Penguin Books, 1993), p. 209.
12 D. G. Haskell, quoted in M. Popova, ‘The Songs of Trees: A Biologist’s Lyrical Ode to How Relationships Weave the Fabric of Life’, The Marginalian, https://www.themarginalian.org/2017/12/08/the-songs-of-trees-david-haskell/; see further D. G. Haskell, The Songs of Trees: Stories from Nature’s Great Connectors (London: Penguin Books, 2018).
13 S. Simard, D. Perry, M. Jones, D. Myrold, D. Durall and R. Molina, ‘Net Transfer of Carbon between Ectomycorrhizal Tree Species in the Field’, Nature, 388 (1997), 579–82, https://doi.org/10.1038/41557. See also Simard, Finding the Mother Tree.
14 On Globalton and Localton, see Chapter Seven.
15 R. Frost, ‘The Road Not Taken’, ll. 1–5.
16 P. Levi, Other People’s Trades (London: Sphere Books, 1990).
17 J. R. Oppenheimer, Science and the Common Understanding (Oxford: Oxford University Press, 1954).
18 Susskind and Susskind, Future of the Professions, p. 307.
19 Ibid., p. 308.
20 I. Berlin, The Hedgehog and the Fox (London: Weidenfeld and Nicolson, 1953).
21 M. Syed, ‘Piers Morgan’s Idiotic rants Reduce Subtle Arguments to Soundbites’, The Times (24 January 2021), https://www.thetimes.co.uk/article/piers-morgans-idiotic-rants-reduce-subtle-arguments-to-soundbites-d2zpchbjv
22 Quoted in R. Jahanbegloo, Conversations with Isaiah Berlin (London: Peter Halban, 1992), pp. 188–89.
23 M. King, The End of Alchemy: Money, Banking and the Future of the Global Economy (New York: W. W. Norton and Company, 2016).
24 Ibid., blurb.
25 R. Lane Fox, The Invention of Medicine: From Homer to Hippocrates (London: Penguin Books, 2020).
26 Whitehead, Adventures of Ideas, p. 25.
27 King, End of Alchemy, p. 367.
28 ‘The Second Coming’ (1919), l. 4.
29 ‘The Rock’ (1934), ll. 6–9, 15–17.
30 Lane Fox, Invention of Medicine.
31 Whitehead, Adventures of Ideas, p. 25.
32 ‘Celebrating G. Octo Barnett, MD’, Journal of the American Medical Informatics Association, 27.8 (2020), 1187–89 https://doi.org/10.1093/jamia/ocaa170
33 E. P. Hoffer, M. J. Feldman, R. J. Kim, K. T. Famiglietti and G. O. Barnett, ‘DXplain: Patterns of Use of a Mature Expert System’, AMIA Annual Symposium Proceedings (2005), 321–24.
34 E. P. Hoffer, G. O. Barnett, B. B. Farquhar and P. A. Prather, ‘Computer-Aided Instruction in Medicine’, Annual Review of Biophysics and Bioengineering, 4.1 (1975), 103–18.
35 K. Ahmed, D. Ingram and C. J. Dickinson, Software for Educational Computing: A General-Purpose Driver for Computer-Assisted Instruction, Interrogation and System Simulation (‘MACAID’) (Lancaster: MTP, 1980).
36 D. de Rougemont, Penser avec les Mains (Paris: A. Michel, 1936).
37 Wiltshaw, E., A History of the Royal Marsden Hospital (Middlesex: Altman, 1998).
38 F. P. Brooks Jr., The Mythical Man-Month: Essays on Software Engineering (New Delhi: Pearson Education, 1995).
39 J. Milan, C. E. Munt and M. W. Dawson, ‘A Model Based Approach to the Evolutionary Development of a High Performance Hospital Information System’, in Medical Informatics Europe ’90, ed. by R. O’Moore, S. Bengtsson, J. R. Bryant and J. S. Bryden, Lecture Notes in Medical Informatics (Berlin: Springer-Verlag, 1990), pp. 457–61.
40 As I completed the book manuscript in March 2023, Thomas told me that he and Stan have joined together in a not-for-profit company called Graphite, which is backed by the US health care providers: Kaiser Permanente, Intermountain Healthcare, Presbyterian and SSM Health. It will build on the Intermountain Clinical Element Models (CEM) as the basis of a trusted and open lingua franca of health care systems. The mission sounds to have much in common with that of openEHR and I hope that may prove the case. The CEM idea is closely analogous to that of the Marsden/GEHR/Synapses/openEHR clinical data object dictionary and openEHR archetype ideas that evolved from the 1980s. Thomas’s stellar contributions to this history, now to be pursued within Graphite, places him in a pivotal position to help further anchor the coherence of the health informatics domain, as a global public good and moving forward as a community interest endeavour, under international governance. As an interesting aside, I noticed the carbon ring hexagon of graphite used in the Graphite company logo. The 1992 GEHR project motif, as I created and used it in presentations and brochures of those times, was also hexagonal and emotive of the hexagonal ring of six carbon atoms in graphite (see Chapter Eight and a Half).
41 Bill read Natural Sciences at the University of Cambridge and then Medicine. Before moving to Moorfields, he had worked at Bart’s, although our paths did not cross there. I well remember one of our lunch time meetings at the Senior Staff Common Room of UCL, where he took out his diary and showed me an entry: ‘Today is the day I was due to retire’, said this young and vigorous person, looking not a day over fifty! He told me that, on leaving Cambridge, he had written the date in his forward diary, anticipating sailing adventures to follow, very well ahead of time! He clearly planned life in great and practical detail! To my relief, he went on to say that he had decided to postpone this plan because our collaboration on OpenEyes was proving such fun and other things could wait. In the event, after some years of intensive involvement, the Moorfields Trust management became uncertain about OpenEyes and recruited some IT consultants, who succeeded only in rocking the boat further. This disturbed even Bill’s sturdy sea legs. He jumped ship and his and his wife’s long planned-for life on the ocean wave came back on track, on a huge catamaran that they bought and christened Double Vision. This is their current odyssey of incremental voyages and explorations in circumnavigating the globe, to be completed before grandparent ties take hold. Judging by Bill’s podcasts, it has involved some of the same mixture of adventure and danger that Odysseus experienced!
42 As further described in Chapter Nine, it had been part of the expectation implicit in my recruitment to UCL that I would engage with change in all these dimensions, and this took much time and energy, alongside the work of building and supporting the team for my new Centre’s academic mission. It was not my responsibility to run the related disparate services, but I was given authority to engage with them and help chart a way forward. Being seen as a flag carrier for such contentious, and often fought over and disruptive, domains as information services and health informatics placed me in the front line of many personal and institutional rivalries, both within the University and in its relationships with local and national NHS organizations and communities. I must have done quite well because several years later I was given a considerable promotion by the Provost and Dean. One eminent but still quite young head of a major clinical division that I had to negotiate with, told me that were it any other colleague coming with the request to join in with a collaborative approach to biomedicine IT support services, he would have distrusted the motivation and feared the consequences for his own research mission, and would therefore have likely stood out against the plan. There are advantages in being an outsider and not engaged in the usual battle ground for status and resource that tend to characterize university communities!
43 Over the past year, I have been working with a local optician in my global village life, who has pioneered an innovative technology called StyleEyes, for producing and customizing prescription spectacles at very low cost. The technology can be used to fit spectacles for users anywhere in the world, by a technician trained to test eyesight and customize the spectacles, in a single visit. This week as I write, my lifelong friend Chris Mullard is discussing with governments and investors in Africa, during one of his regular visits there as a UK business ambassador, to explore how StyleEyes might now be brought to life by investors there.
44 ‘Constitution’, WHO, https://www.who.int/about/governance/constitution
45 The poem is entitled ‘Something Clicked’. See BT, ‘Something Clicked by Simon Armitage, in Partnership with BT’, online video recording, YouTube (1 Oct 2020), https://www.youtube.com/watch?v=kQS3k3yBxAk
46 A. N. Whitehead, Adventures of Ideas (New York: Macmillan, 1933), p. 108.
47 A. Einstein, Ideas and Opinions (New York: Crown Publishers, 1954), p. 271.
48 A. N. Whitehead, The Aims of Education and Other Essays (New York: Macmillan, 1929), p. 4.
49 N. Gershenfeld, ‘Bits and Chips’, New Scientist, 169 (2001), 55.
50 A. Einstein, The Einstein Reader (New York: Citadel, 2006), p. 7.
51 Penrose devised new mathematical methods that enabled him to show the black hole as a firm prediction of the Einstein equations of general relativity. His theory was published in a paper from Oxford, in early 1965, when I can attest there were no computers in sight, anywhere. Genzel and Ghez are astrophysicists, in Germany and the USA, who spent many years from the early 1990s in mapping the movements of stars in Sagittarius A*, at the centre of the Milky Way galaxy, in which we sit. With progressive refinement of both instruments and correction for distortions of images, they demonstrated the presence there of a massive black hole. The mathematics was the product of a brilliant and inventive mathematical brain, with pencil and paper. The astrophysicists’ observations were only made possible by the much later advances in instrument engineering and computational infrastructure. The evidence demonstrating the correctness of Penrose’s prediction, without which it would have remained interesting theory, was also evidence of the central role of this computational infrastructure in the creative interaction of mathematics, science and engineering.
52 HIMSS, ‘2022: Future of Healthcare Report’ (2022), https://pages.himss.org/rs/420-YNA-292/images/PDF-FOH%20Report-2022-08.pdf
53 T. Sullivan, ‘Why EHR Data Interoperability Is Such a Mess in 3 Charts’, Healthcare IT News (16 May 2018), https://www.healthcareitnews.com/news/why-ehr-data-interoperability-such-mess-3-charts
54 Susskind and Susskind, Future of the Professions, p. 22.
55 Ibid., pp. 37–38.
56 I should note at this point that my knowledge and experience of the practical skills and professions of surgery and invasive procedures, more widely, are very limited, although I have observed them at close quarters and worked alongside their practitioners. These are domains where unfolding information technology and engineering—image guidance and robotics, for example—have been transforming practice and likewise education and training. I will not delve into the separate considerations in play in investment, assessment and regulation of these professional skills, and how they may evolve and impact the health care professions as such tools and devices acquire greater scope and usability in the years ahead. They will be an important aspect of the transition towards more citizen-centred health care.
57 D. Black, ‘Data for Management: The Körner Report’, BMJ (Clin Res Ed), 285 (1982), 1227–28, https://doi.org/10.1136/bmj.285.6350.1227
58 Susskind and Susskind, Future of the Professions, p. 45.
59 Ibid., p. 412.
60 Whitehead, Aims of Education, p. 97.
61 M. Beckman, Math without Numbers (New York: Penguin Books, 2022).
62 I. Illich, Deschooling Society (London: Calder & Boyars, 1971), p. viii.
63 Ibid., p. 113.
64 According to legend, Prometheus stole fire from the gods and gave it to humanity, interpreted as a gift in the form of technology, knowledge and civilization, aiming to cure human ills but betimes leading to overreach and unintended consequence. There are several stories about how Zeus, the king of the gods, took vengeance by condemning Prometheus to eternal torment and presenting Pandora to Prometheus’s brother Epimetheus. Pandora opened a jar (or box, as it became known) left in her care and out of it came sickness, death and other evils that spread into the world. Only hope, or in a pessimistic translation of the Greek, ‘deceptive expectation’, remained when she hurriedly closed the jar.
65 Illich, Deschooling Society, p. 115.
66 Ibid., p. 107.
67 Ibid., p. 111.
68 Ibid., p. 115.
69 J. Barnes, A History of the World in 10½ Chapters (New York: Knopf, 1989).
70 Congress of the United States Office of Technology Assessment, Computer Technology in Medical Education and Assessment (Washington, DC: Congress of the United States Office of Technology Assessment, 1979), p. 5, https://www.princeton.edu/~ota/disk3/1979/7903/7903.PDF
71 Topol, Deep Medicine.
72 Ibid., p. 18.
73 Ibid., p. 31.
74 See ibid., p. 29.
75 Ibid., p. 20.
76 Ibid., p. 21.
77 Ibid., p. 56.
78 Ibid., p. 94.
79 Ibid., p. 92.
80 Ibid., p. 94.
81 Ibid., p. 50.
82 Ibid., p. 52.
83 Quoted in ibid., p. 82.
84 Quoted in ibid., p. 82.
85 Ibid., p. 310.
86 G. Tett, Anthro-Vision: A New Way to See in Business and Life (New York: Simon and Schuster, 2021).
87 The lawyer who led the preparation of the legal framework of the Community Interest Company (CIC) in the UK, Stephen Lloyd, was a fellow trustee of mine in the charity, StartHere. This pioneered an information system and kiosks where citizens could readily access information about local and global support services available to them, to provide help and support when they did not know where to turn. This was, essentially, an example of a prototype citizen-centred information utility. It struggled to gain traction, in large part, it seemed, because of the fears of existing groups and interests that did not wish to have their perceived ownership of individual channels of communication usurped or destabilized, and others who saw themselves as the rightful owners of responsibility to integrate them, in different contexts. Like the APoGI project of CHIME at UCL, discussed above in context of Bernadette Modell’s pioneering vision, it sought to provide a single point of access and a manageable balance and continuity of information provided, configured to suit different audiences. I describe StartHere and its founders and motivational leaders, Sarah Hamilton-Fairley and Richard Crofton in Chapter Nine. I tried, and failed, to gain traction between this kind of information service and the openly standardized care records approach I was helping to pioneer in the openEHR care records platform and OpenEyes, as featured in Chapter Eight and a Half. The industries and services of the day fought to preserve their fragmented identities and associated silo information environments, albeit often to the detriment of the communities served, that became easily overwhelmed by the complexity involved in navigating the non-coherent information environments that prevailed. Lloyd’s law firm, Bates Wells & Braithwaite, helped me hugely, in later years, in steering the transition of the globally expanding operations of the openEHR Foundation, into the framework of the self-governing openEHR International Community Interest Company (CIC).
88 ‘The Second Coming’ (1919), l. 3.
89 T. S. Eliot, ‘The Waste Land’, l. 1.
90 M. du Sautoy, The Creativity Code: How AI Is Learning to Write, Paint and Think (Cambridge, MA: Harvard University Press, 2019).
91 Weizenbaum, Computer Power.
93 NHS Executive, Priorities and Planning: Guidance for the NHS 1996/97 (Leeds: HMSO, 1996).
94 D. Ingram, R. V. H. Jones, I. Finlay and A. Lant, ‘An Interactive Videodisc “Cancer Patients and Their Families at Home”, Designed for Education in Primary Health Care’, Journal of Audiovisual Media in Medicine, 15.2 (1992), 73–76.
95 F. Rosleff, European Healthcare Trends: Towards Managed Care in Europe (London: Coopers and Lybrand, 1995).
96 D. Graeber, The Utopia of Rules: On Technology, Stupidity, and the Secret Joys of Bureaucracy (New York: Melville House, 2015), p. 89.
97 K. Popper, The Open Society and Its Enemies: The Spell of Plato (London: Routledge and Kegan Paul, 1957), p. xxxvii.
98 N. Davies, Europe: A History (Oxford: Oxford University Press, 1996), p. 46.
99 N. Davies, Heart of Europe: A Short History of Poland (Oxford: Oxford University Press, 1984).
100 IXN is a network of university computer science departments, collaborating on project assignments for students, as part of their taught course. Created and led by my UCL colleagues Dean Mohamedally and Graham Roberts, it has proven mutually beneficial for health care research and development teams and the many thousands of undergraduate and postgraduate students studying computer science. They are collaborating on ambitious projects involving novel new clinical applications. One such has been to bring AI software into assessment of eye disease, linking with clinicians and system developers of the OpenEyes ophthalmology medical record system.
101 King, End of Alchemy, p. 343.