



6. The mill that grinds young people old
© 2018 Daniel Nettle, CC BY 4.0 https://doi.org/10.11647/OBP.0155.06
One and the same cause
Wears out our bodies and our clothes
–Bertolt Brecht, A worker’s speech to a doctor
I am in the cemetery again. It’s a good place to meditate on the conditions of life, and on the relationships between biology and social science. This is the cemetery of ‘neighbourhood B’, one of the fieldwork sites of my ethnographic project Tyneside Neighbourhoods.1 That project was about life. Here I am reflecting on ageing and death.
Neighbourhood B is in Newcastle upon Tyne. Walking distance from two huge universities, from a large teaching hospital, a cycle ride from offices of regional and national government, it is nonetheless one of the most deprived places in Britain. People working in dangerous heavy industries lived and died here. Later, the neighbourhood atrophied along with the industries that bore it. Its population declined and its future became unclear. It is not a bad place. It persists quietly because there is nothing else it can do, persists despite stagnation and economic precariousness for its residents, squalor in its structures, and ever-greater retrenchment of its public services. The cemetery is an odd mixture of municipal decline and gaudy activity. The fine mausoleum and other elaborate Victorian buildings are all falling down. Maintenance is limited to some movable iron fencing panels to keep people out. Pigeons roost in collapsing roofs. The older headstones have fallen over, or else been laid down before they injure someone. But many of the younger headstones—black marble and gilt—are islands of activity in the grass. Fading children’s bears, balloons, photos, withering flowers, hand-written messages—some of these on the graves of people who died twenty or even thirty years ago.
The place is written through with human biology, for what could possibly be more biological than the cessation of our organismality, the cessation of all of those metabolic and physiological processes that make us someone rather than an inanimate object? Yet this is also a place rich in social meaning and social pattern. This is not an accidental coupling, some unlikely final juxtaposition of two worlds—the ‘social’ and the ‘biological’—that in life flow separately, have little fundamentally to do with one another. This place derives its social meaning from the very fact that death (and therefore life) is a biological process. Its social meaning is incomprehensible if not grounded in that fact. That is what brings the mourners with their balloons and their bears, the undeniable and impassive biology of the situation. But though these deaths were biological events, their determinants (or the determinants of their immediate determinants) belong very clearly in the domain of the social. Here in the cemetery, there is no space between the biological and the social. The graves mark their indissoluble unity, which was as true in life as it was in death.
§
Wandering around, I am struck how many of these people died young. Here’s Susanna E., died at 44; Gemma G., aged 10; Jay R., clearly a big Newcastle United supporter to judge from his headstone, aged 19. Here’s Paul C., dead at 33, next to his dad James, dead a couple of years earlier at age 55. There are several graves of babies. Life round here seems, if not nasty and brutish, then certainly short. Of course, I could be guilty of confirmation bias, of noticing the stand-out young ones. So I get interested and start to collect some data.
I complete a survey of the graves dating from 1990 onwards, noting sex and age at death. It is not perfect, since I get lost crossing and re-crossing the cemetery, and some more recent deaths are put into older established family graves, confusing the inclusion criteria. Still, I end up with a sample of nearly 200 deaths. With this sample I can estimate the probability density function for age at death. What this function tells you is not the probability of dying at any particular age (you would need data from the living for that). What it tells you is, given that you died, the probability of being any particular age at the time. This is a relevant consideration for life; we’ve all got to die at some age, and it would be nice to have a sense of the distribution of likelihoods for what that age will be.
The resulting density is shown in figure 1. It looks different for men and women, which we ought to expect. The average age at death is about 61 for men, and nearly 69 for women. 61 years. The current (2014) life expectancy at birth for Afghanistan is 60.2 More important than the low average is the variability in ages at death. As a man from round here, it is most likely that my age at death will be in the 60s, but it could be any age, from the day of my birth onwards. As you can see from figure 1, the likelihood of death coming in my twenties is really not negligible. For the women, late seventies is the most likely time, but again, it could well be earlier (though not as likely to be under 40 as is the case for the men), just as it could be later. A statistic that expresses this imprecision in when we are going to die is the standard deviation of age at death. The mean of 61 says that the average age at death of all the men is 61, but the standard deviation of age at death of almost 20 years says that a typical individual’s age at death is higher or lower than the average by two decades. So you could be 41, or 81, without being in any sense exceptional.
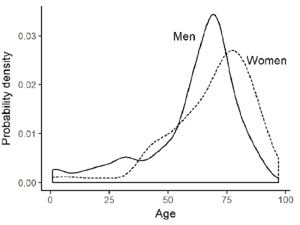
Figure 1. Estimated probability density functions for the male and female ages at death in Neighbourhood B cemetery, graves established since 1990, survey of January 23rd 2017.
This is all very atmospheric, you might say, but not very scientific. This is one cemetery with no comparison data. Not everyone who dies is buried here; maybe there are biases towards memorializing those who died young. Quite right of course, but the cemetery is just an illustration of something we know to be true from much more systematic national data. Poor people die relatively young in contemporary Britain. The size of the disparity depends a little how you do the calculation. If you do it by individual social class, it is probably around 6 years for men and 5 years for women.3 If you do it by place, comparing not individuals by their occupation, but communities by their overall levels of deprivation and want, the disparities are more like 8 and 6 years.4
§
We first meet Paris, in Dickens’s A Tale of Two Cities, in an extraordinary passage at the beginning of Chapter 5. In the neighbourhood of St. Antoine, a cask of wine has been dropped and broken in the street. Suddenly, there are the inhabitants, scooping wine with their hands from between the cobble stones; making dams out of mud to drink the resulting pool; mopping wine up with handkerchiefs to squeeze into the mouths of their infants; even champing on wine-rotted fragments of barrel. They leave whatever they were doing, the painful drudgery of their daily lives, in mid-action, for a transitory wine frolic, an expected carnival.
The people of St. Antoine, Dickens tells us, had undergone a terrible grinding and re-grinding in the mill of poverty. But what kind of mill is the mill of poverty? Dickens: ‘The mill which had worked them down, was the mill that grinds young people old’. The mill of poverty is a mill of ageing: the effect of poverty is to age you faster. This is an important idea, not least because it suggests how an intuitively ‘internal’ and ‘biological’ process, ageing, is profoundly affected by the indubitably ‘social’ processes of deprivation and inequality happening beyond the body envelope.
§
I want to take Dickens’ analysis of St. Antoine seriously, in two ways: first, the effects of poverty should be considered as ageing; and second, that the spontaneous frolic with the windfall of wine—the behaviour of the residents of St. Antoine—is somehow systematically connected to the ageing effects of poverty.
What evidence could we adduce in support of the idea that the effects of poverty constitute ageing? We need to define what ageing is. Biologists define ageing as the deterioration of an individual’s biological performance over his or her life. Influential current theories of ageing suggest that this decline is due to the accumulation, in the body, of unrepaired damage.5 DNA becomes oxidated and unreadable; key populations of stem cells lose capacity; mechanisms lose their shape and capacity to rebound; all due to the continuous assaults of chemistry and physics upon our bodies. There is no internal ticking clock; organisms are not programmed to self-destruct after some particular delay. For this reason, the pace of ageing can vary wildly from individual to individual.6 It is not time per se that it is doing the work: it is the net effect of the rate at which damage accumulates, and the activities of the body to repair it.
So what evidence is there that poverty can accelerate ageing? Well, there is no greater decline in biological performance than becoming dead, so in one sense, if death comes earlier for poor people (and we have already seen that it does) then ageing is by definition faster. But we can see it clearly in declines in performance short of death, what medics call morbidity, as well. Poor people are in worse health than rich people at all ages, but importantly their health goes downhill with time more rapidly through adulthood. We can distinguish statistically between expectancy of life—the number of years you can expect to be alive at prevailing rates of mortality—and expectancy of health, which is the number of years of good health you can expect to have at prevailing rates of morbidity and mortality. Whilst the life expectancies of poor English communities are 6–8 years less than those of rich ones, the health expectancies are nearly 17 years less, for both sexes.7 In the most deprived English neighbourhoods, health expectancy is only about 50. In my neighbourhood B, fully one third of 18–65 year olds have a serious longstanding health problem.8 Deprivation and the deterioration of physical health as the years go by are so closely associated that you could almost use the latter as a measure of the former.
It is not just medical symptoms that show an effect of poverty: it is also underlying physiological processes. There is increasing interest in the idea that we should measure people’s biological age (that is, where they are in the inevitable arc of biological performance) rather than just their chronological age, which is a very poor approximation for what is really happening to them.9 We can do so using suites of ‘biomarkers’, namely bodily measurements that have the properties of (a) changing on average with increasing chronological age; and (b) predicting time until death better than chronological age does. One set of such markers measure inflammation. Inflammation is part of our immune response to injury and infection, and such the capacity to mount an inflammatory response is an adaptive one. With age though, the background levels in our bodies of molecules involved in the general inflammatory response increase. The levels of these molecules predict future serious disease better than chronological age does. Thus, inflammation markers in the blood (C-reactive protein and interleukin-6 are the most widely measured) serve as markers of biological age.
Many studies have found that poor people show higher levels of these inflammation markers than rich people, and not just when they are old.10 It’s true in mid-life, decades before most people die, and it is even true in adolescence.11 The study on adolescents examined what it is about the lives of the less privileged that best explained (in a statistical sense of explain) their greater inflammation. The answer is sobering: they experience less happiness.
§
‘If I’d known I was going to live this long, I would have taken better care of myself’ is one of those quips with something so satisfying about it that it ends up attributed to many different people. It makes a kind of sense: the extent to which we orient our behaviour toward the future depends on how likely that future is to ever come about. Indeed, this is one of the key principles of some evolutionary theories of ageing. The mouse that invests so much in repairing its DNA that its DNA would continue to replicate fine for 10 years has probably wasted its effort. In the wild, 90% of mice are gone within 1 year anyway, from predation or cold. So mice have evolved to spend no more on DNA maintenance than necessary; instead, what they are really astonishingly good at is making baby mice while the sun shines. Engineers apparently get it too. An urban legend has Henry T. Ford instructing his engineers to tour the scrapyards of American looking for parts of his cars that never wore out. They found that the king-pins of the scrapped cars invariably still had life in them. His response: make the king-pin less well.12
Now we turn back to the residents of Dickens’ St. Antoine, with their impromptu carnival of the spilt wine. They are conforming to an established stereotype about poor people: they value immediate opportunity (dropping what they were doing to consume during the day) over preparing for the future (the sawing of the wood stands neglected). Gillian Pepper and I recently reviewed the evidence that this stereotype contains a germ of truth: people living in poverty in Western countries do favour the present relative to the future more than their affluent co-citizens, in a number of different ways.13 This orientation to the present is underpinned by a kind of fatalism and a belief in the role of chance. For many commentators these attitudes, these ‘poor choices’, become something to condemn morally, or attempt worthily to educate away, a psychological failing of poor people that is the root cause of their poverty.
But there is another side from which you can look at this. Here in my neighbourhood B cemetery, I ask myself: why not? Say I am a member of the C. family, whose graves I have just been looking at. The dad got 55 years, the son got 33. How much effort would I choose to make in, say, saving for a pension. Neither even reached the statutory pension age. Would I have smoked? Well, nicotine is a stimulant, giving you a pleasant buzz, and the really bad consequence, lung cancer, doesn’t really start to hit until after age 45.14 Half of deaths from lung cancer are in the over 75s. You see the point: a lot of the decisions that poor people make start to make a kind of sense. Gillian Pepper struggled to find a name for this ‘making a kind of sense’. She didn’t want to use the term ‘adaptive’, since this has a technical meaning in biological theory, a technical meaning that was close but not identical to what she meant. She didn’t want to use the term ‘rational’, since this can mean a number of different things, and for many, connotes the result of very extensive conscious deliberation, which she did not want to imply. So she settled on ‘contextually appropriate response’. Living with a bias towards the present is a contextually appropriate response to the reality of poverty. Gillian (and I) are agnostic about whether this response is extensively reasoned through, or more automatic and sub-conscious, or a bit of both.
The best worked-through case of contextual appropriateness is the age of childbearing. The really big difference between the rich and the poor in Britain is not in how many children they have, but in when they have them. On average, this differs by at least a decade between the richest and poorest districts.15 We can see this very clearly in the cemetery. Here’s the grave of Nora W., dead at 23 but already a mum; Maureen O., dead at 49 but already a nana (grandma); Tommy D., dead at 62 but already a great-grandfather. You have to get on with it to keep the generation time this short. Commentators are fond of morally chastising the poor for their reproductive decisions, and laying all kinds of social ills at the door of early childbearing.16 This is quite unjustifiable: the extremely late reproduction of middle-class people causes far more by way of medical problems and costs.
Instead, let us put the problem the other way around. It’s quite a widespread human desire to hold one’s grandchildren, to care for them whilst one is still hale and living. Those very commentators who lambast teenage mothers would probably endorse this aspiration whole-heartedly. In a paper a few years ago, I entered into the following thought experiment: Say I was a young woman and wanted to be able to expect, assuming my life and that of my daughter followed the average trajectory, to be alive and in good health until my oldest grandchild was five years old. When would I need to start childbearing? The answer for the poorest decile of English neighbourhoods: about 22. And that is almost exactly the age when people in those neighbourhoods do start childbearing, on average. As Arline Geronimus argued in a classic paper from years ago, young women who live lives of deprivation seem to know what they need to do, and so they do it.17
What about if I live in the median English neighbourhood? 28. Again, that’s about what people actually do. And if I lived in the most affluent neighbourhoods? I could wait until after 30. And look; there we are. Enormous demand for IVF and egg-freezing, coming from rich neighbourhoods, because the rising health expectancies of the rich have prolonged the contextually appropriate schedule. That’s fine; but let us not stigmatise the contextually appropriate behaviours of those who have to live their lives under different circumstances.
§
Isn’t there a horrible circularity to this whole argument? You say that the poor smoke, don’t adhere to medications, bear children young, and eat badly because they won’t be alive long enough to see the negative consequences of these behaviours. But surely, the reason they won’t live so long is exactly that they smoke, don’t adhere to medications, eat badly, etc. So you seem in some way to be explaining their lifestyle by their lifestyle, which does not seem very satisfying.
This objection should not be hastily dismissed. When we do epidemiological studies of the relationship between social class and health or mortality, we always find that poor people fare worse than rich. Some of this is indeed because they are more likely to smoke. So you control statistically for smoking. Some of it seems to be due to poorer diet. So you control for diet. Some of it seems to be due to patterns of physical activity. So you control for physical activity. And it’s true, the burden of excess mortality and morbidity is reduced by controlling for these things, maybe reduced by about a half. It is not reduced to nothing, though. However many voluntary behavioural things you control for, there is always a residuum of excess mortality and morbidity hanging over poor people. This, Gillian Pepper and I would argue, is the structural bit, the bit fundamentally due to too few material resources and too many demands, the bit that poor people cannot control except by not being poor (and if they had an available option of not being poor, we assume they would mostly take it up).
Our argument turns on this structural bit of health risk, this uncontrollable bit, being substantial. This structural excess health risk due to poverty is like predation and cold for wild mice; just there as part of the ecology, to be adapted to rather than opted out of. And you adapt to it by rebalancing between present and future consequences. Many of the arguments between left and right over the consequences of poverty are about the relative importance of the structural-ecological bit and the voluntary-behavioural bit of health risk. On the right, we decry people for being irresponsible, for not making better choices, not getting on their bikes to improve their lives. On the left, we are prone to point to structural sources of disadvantage, and invoke the criticism of having a victim mentality. The truth is that both bits are important. The account Gillian and I outline, though, hands an explanatory primacy to the structural-ecological bit. The presence of this structural increase in mortality and morbidity risk reduces the payoff for voluntary investments like adhering to medical recommendations, avoiding smoking, and so forth, and increases people’s relative valuation of present enjoyment.
The voluntary-behavioural bit is important, though. In fact, it is responsible for a cruel irony I dubbed in an earlier paper the ‘exacerbatory dynamic of poverty’.18 Because of their structural-ecological disadvantage, the poor have less incentive than the rich to invest in their future health; but then the consequence of this reduced investment is to widen the health gap between the two groups to more than it structurally needs to be. And if the voluntary-behavioural choices of one generation partly determine the structural-ecological situation of their children, then we have scope for an inter-generational system of disadvantage that can self-perpetuate, and is hard to unravel. What is pretty clear, though, is that just putting larger warning labels on cigarettes and sweet foods is much like improving the sign-posting to the lifeboats on the Titanic. It is naïve for policy-makers or anyone else to assume otherwise.
§
Dickens’ description of St. Antoine is characteristically evocative. Hunger and deprivation is written into the visual environment—in the ancient faces, the inadequate clothing, the dilapidation and litter, the poor foods on sale. All of these serve as ‘grim illustrations of Want’. It is 240 years since the time Dickens was writing about, and 160 years since he wrote, but as I stroll around neighbourhood B, I muse on how little has changed. I instantly know that this is a poor neighbourhood, from the terrible litter, the state of the buildings, the clothes people wear, the things they are doing, as well as the headstones in the cemetery. The environment seeps information; information stares down from the chimneys, starts up from the kerb; it is written in the shops, the houses, the gardens.
In recent years I have become interested in the information that is freely available just by being somewhere. For me as a researcher, it is a resource. These days we under-do the simple acts of observation, the collection of this free information, which is why I am frequently to be found here counting passers-by, documenting whether doors are open or closed, tabulating litter or recording ages from headstones. These simple acts get neglected in an era of standardized surveys, controlled experiments, big data, focus groups, and discourse analysis. This is a shame—whatever your research predilections, it seems to me that the point of departure for research should always be the organism in its environment. Indeed, the organism in its environment (or individual in their context) is a shared starting point that unites behavioural biology and social science. So you can’t do much better than put yourself in the environment, and ask: what do my study subjects see every day? What do they hear? What do they smell? Collect the information they collect, and it might help you begin to understand what they feel, why they do what they do.
It is not just the researcher who needs to harvest information. It is the study subject too. We come into this world with, within important limits, fairly open priors about what it will be like. So we have to detect our local environment, and cut our behavioural cloth accordingly. For this reason, characterizing the types of information available to the organism, the cues it can use to calibrate itself, is an important theoretical focus in behavioural biology.19 I would like to see more explicit consideration of it in social science research too: the precise quantification of the information freely available to people in their daily lives, in their ordinary social environment. We know that poor people have different attitudes about the future than the rich, and Gillian and I have argued that these attitudes are contextually appropriate. But how do people know what is the correct attitude to develop for their particular ecology?
They are taught it, one might say. People tell them how they should behave. Or they imitate. Well, maybe, to a point. But I think there is a far greater role than we usually acknowledge for non-verbal inference based on sensory cues in the material environment. We know this is how visual perception works. What we receive is a set of cues of contrasts, surfaces and edges; what we infer is a world of objects and motion. By the same token, when we walk around neighbourhood B we see second-hand shops and litter and the mausoleum falling down (and, one morning as I ambled by, a wash-basin come crashing out of a closed upstairs window); what we receive is information. This is what life is like, will be like in the future. It doesn’t need explicitly saying, or teaching, or pointing out. It is there, and you can no more not receive it than you can avoid perceiving a football as continuing to exist when it rolls behind a parked car.
This brings me back to the graves where I started. Every one of these deaths was a meaningful cue, never forgotten, to the living: to sons, daughters, siblings, friends. That’s what could await me. Gillian carried out a study where she showed that more experience people had of bereavement, the more they devalued the distant future, and the sooner they wanted to start a family.20 This makes perfect sense. The living can harvest information from death.
Perhaps this can answer another puzzle for us: the extraordinary elaboration of death in neighbourhood B. Although the cemetery itself is neglected and gracelessly dilapidated, many individual graves are tended and celebrated to a striking degree. Marble headstones that look remarkably expensive feature photographs, engravings of caravans, or pet dogs, or Newcastle United shirts. The flowers, balloons, bears, reindeer and cards are clearly renewed. And it is not just within the cemetery. It is very common as one walks around the West End to find flowers and cards tied to lamp-posts, railings or benches. Someone fell here. Someone loved this spot. I have not done a systematic study, but I don’t believe you would find this degree of attention to death in a more affluent area.
There is only one conclusion you can come to: these deaths mean a lot round here. What does it mean for something to mean something? That’s a rather involved philosophical question, but there are deep conceptual links between meaning, information, and uncertainty. A death means a lot if it carries a lot of information. And a death can only carry a lot of information if there is something about death we are uncertain about. For example, if every person died on the morning of their 79th birthday, there would be no information in age at death. We would be under no uncertainty about it. We would not say ‘taken from us too soon’ or ‘sudden and unexpected loss’. We would not be shocked. But we have seen that in this cemetery, the standard deviation of age at death is 20 years. In other words, there is a lot of variation, probably more variation than would be true in an affluent place. Hence the neighbours live under uncertainty about when they are going to die. As a result, every death is informative. And when something is informative, you look at it for longer. You remember it for longer. You keep coming back here.
1 Nettle, D. (2015). Tyneside Neighbourhoods: Deprivation, Social Life and Social Behaviour in One British City (Cambridge: Open Book Publishers), https://doi.org/10.11647/obp.0084, https://doi.org/10.11647/obp.0084
2 Information from http://data.worldbank.org/indicator/SP.DYN.LE00.IN
3 Trend in life expectancy at birth and at age 65 by socio-economic position based on the National Statistics Socio-economic Classification, England and Wales: 1982–1986 to 2007–2011. Office for National Statistics statistical bulletin released 21st October 2015. Downloadable from www.ons.gov.uk.
4 Inequality in Health and Life Expectancies within Upper Tier Local Authorities: 2009 to 2013. Office for National Statistics statistical bulletin released 20th November 2015. Downloadable from www.ons.gov.uk.
5 Kirkwood, T. and S. Austad. (2000). Why do we age? Nature 408: 233–8, https://doi.org/10.1038/35041682
6 Belsky, D. W. et al. (2015). Quantification of biological aging in young adults. Proceedings of the National Academy of Sciences 112: E4104–10, https://doi.org/10.1073/pnas.1506264112
7 Figures from Inequality in Health and Life Expectancies within Upper Tier Local Authorities: 2009 to 2013. Office for National Statistics statistical bulletin, released 20th November 2015. Downloadable from www.ons.gov.uk.
8 Nettle, D. (2015). Tyneside Neighbourhoods (Cambridge: Open Book Publishers, p. 115), https://doi.org/10.11647/obp.0084, https://doi.org/10.11647/obp.0084
9 Levine, M. E. (2013). Modeling the rate of senescence: Can estimated biological age predict mortality more accurately than chronological age? Journals of Gerontology, A 68: 667–74, https://doi.org/10.1093/gerona/gls233
10 E.g. Gruenewald, T. L. et al. (2010). Association of socioeconomic status with inflammation markers in black and white men and women in the coronary artery risk development in young adults (CARDIA) study. Social Science and Medicine 69: 451–9, https://doi.org/10.1016/j.socscimed.2009.05.018; Koster, A. et al. (2006). Association of inflammatory markers with socioeconomic status. Journals of Gerontology A 61: 284–90, https://doi.org/10.1093/gerona/61.3.284; Nettle, D. (2014). What the future held: childhood psychosocial adversity is associated with health deterioration through adulthood in a cohort of British women. Evolution and Human Behavior 35: 519–25, https://doi.org/10.1016/j.evolhumbehav.2014.07.002
11 Chiang, J. et al. (2015). Socioeconomic status, daily affective and social experiences, and inflammation during adolescence. Psychosomatic Medicine 77: 256–66, https://doi.org/10.1097/psy.0000000000000160
12 This story can be found in many places, but was probably introduced into the folk culture of biology by Humphrey, N. (1976). The social function of intellect. In Growing Points in Ethology (P. P. G. Bateson and R. A. Hinde eds., Cambridge: Cambridge University Press, p. 303–17).
13 The evidence is reviewed in Pepper, G. V. and D. Nettle. (2017). The behavioural constellation of deprivation: Causes and consequences. Behavioral and Brain Sciences 40: e314, https://doi.org/10.1017/s0140525x1600234x
14 See: http://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/lung-cancer/mortality#heading-One
15 Nettle, D. (2010). Dying young and living fast: variation in life history across English neighborhoods. Behavioral Ecology 21: 387–95, https://doi.org/10.1093/beheco/arp202
16 In the UK, early childbearing was a media and public policy obsession for a while, and then just as mysteriously dropped out of interest. See Arai, L. (2009). Teenage Pregnancy: The Making and Unmaking of a Problem (Bristol: Policy Press).
17 Geronimus, A. T. (1996). What teen mothers know. Human Nature 7: 323–52, https://doi.org/10.1007/bf02732898
18 Nettle, D. (2010). Why are there social gradients in preventative health behavior? A perspective from behavioral ecology. PLoS ONE 5: e13371, https://doi.org/10.1371/journal.pone.0013371
19 See for example McNamara, J. M. et al. (2016). Detection vs. selection: Integration of genetic, epigenetic and environmental cues in fluctuating environments. Ecology Letters 19: 1267–76, https://doi.org/10.1111/ele.12663; Frankenhuis, W. E. and K. Panchanathan. (2011). Balancing sampling and specialization: An adaptationist model of incremental development. Proceedings of The Royal Society B: Biological Sciences 278: 3558–65, https://doi.org/10.1098/rspb.2011.0055
20 Pepper, G. V., and D. Nettle. (2013). Death and the time of your life: Experiences of close bereavement are associated with steeper financial future discounting and earlier reproduction. Evolution and Human Behavior 34: 433–9, https://doi.org/10.1016/j.evolhumbehav.2013.08.004

